Previous Chapter ... ... Next Chapter
Prehabilitation is an extension of rehabilitation. Typically, prehabilitation is referred to "pre-" rehabilitation" or doing rehabilitative work before you acquire an injury. However, the way I think it is best thought of in the context of pre-injury or post-injury rehabilitation state: there is the awareness of discomfort in certain muscles, connective tissues, or joints but there is no presence of pain or actual injury.
In my opinion, it is more natural to think of it like this because we will pass through a similar stage whether we acquire an injury or not. Thus, we look at and identify whatever is the cause of a pre-injury or post-injury state such as imbalances, weaknesses, overuse, or other factors. After we analyze this, we need to be proactive in either correcting those imbalances, strengthening, or resting to bring the tissues and joints back into a more healthy and normal state.
Therefore, prehabilitation is used for two distinct reasons.
The firstis the extension of rhabilitation where one previously had an injury such as tendonitis. In this example, the tendonitis is currently rehabbed to the point that there is no more pain, but excessive volume or intensity on the area may reinjure it. The area is vulnerable to injury. The area may need to be programmed around for general training
The second is the state of pre-injury. It is better to catch the injury before it devolves into pain, muscle atrophy, and other negative consequences and work on it before to restore the tissues to a normal state. Typically as stated before the ues are tending to be "underrecovered" or "overworked" such that there is discomfort without pain or there may be twinges of pain. This is where we want to back off and reassess what we are doing 50 as to correct this.
There are five main areas of the body that I am going to discuss in regards to upper body training. These are the hips, spine, shoulders, elbows, and wrists. These joints and the surrounding musculature are the main areas in bodyweight exercises that we need to take care of to make sure nothing happens to them. These will also be discussed in the next section on mobility and flexibility.
Prehabilitation is often about correcting imbalances or improving dysfunction tissues which is why a Tot of what is going to be talked about in this chapter is based behind the previous chapters on injuries.
This is the main time I like isotonic (same rate of movement) exercises in conjunction with eccentrics (muscle lengthening) as the main types of movements for prehabilitation. Isolation type exercises may be used specifically to work on imbalances or target tissues that may need extra work.
Typically, this type of work will be an extension of rehabbing back from injuries which means you can use the same exercises that you were given by your doctor or physical therapist. However, if you are approaching this from the pre-injury state of things that is good. We never want to have a full blown injury as pre- rehabilitation work is much easier to to than post- rehabilitation.
I am going to talk about mobility and flexibility as a whole next, and then we will focus in on general solutions as each of these things are interrelated with each other.
The definition of mobility is the ability to move freely. We can use flexibility training to increase our mobility, and we can use other techniques such as massage or full range of motion exercise to help break up soft tissue adhesions or increase range of motion as well
As such, mobility can be thought of as a bridge between prehabilitation and normal quality of movement that we would be using to performing our strength movement.
Our goal is to get the range of motion (flexibility). Then be able to move within that range of motion (mobility). Then be able to improve strength or endurance within that movement (isolation — compounds) to work back into full strength work.
Flexibility work itself is an important part of bodyweight strength training especially in some of the variations of skills such as the straight arm press handstands and L-sit/V-sit/manna variations. However, like I have talked about before in the core work section, the thing we are all working towards is what we like to call "active flexibility."
Active flexibility takes advantage of using the muscles in the active insufficiency (or shortened range of motion) where we are operating at the limits of our flexibility. This requires a great amount of strength and control. This type of strength work which is mostly for the shoulders and hips must be developed in conjunction with mobility and flexibility work as well.
We do not want to work these things for the sake of working them. We always need to have a goal or overarching theme behind why we want to have that extra range of motion or mobility.
There are two prevailing popular methods of thought out there in regards to common injuries. The first 1am sure that everyone know is "no pain no gain." While this applics great to aspects of training such as metabolic conditioning, it does not scale well with injuries. The other line of thought is rest, rest, and more rest. While rest is good it depends on what kind of rest is implemented. Often the truth is somewhere between each of these two lines of thought.
So why are mobility and flexibility so important?
1 think the most underused example is the use of mobility in the context of how good it is for our joints. Take for instance the fact that hip replacement is becoming extremely common in the United States. Joint replacements occur because our joints become "unhealthy" from lack of movement. Thus, they start to develop arthritis and other painful maladics.
The main oceupational thing that has become prevalent with people working jobs in the US is desk work. That i to say that people are sitting down 8+ hours per day and not moving their hips at al.
Anyone can tell you that what happens when you break a bone and you are put in a cast that your muscles start to atrophy, joints start to become stiff, and your connective tissues become weaker. The same thing occurs with self imposed semi-restrictions such as with padded shoes (akin to soft casts), and restrictions just imposed by working such as sitting.
Movement in general is good for our joints, connective tissues, and muscles which is why in previous chapters I rarely recommended straight up rest for an injury. Doctor who recommend straight up rest are incorrect as well. The only time "rest" should be indicated is if someone does not know specifically how to rehabilitate something or they are overactive and overcager with their training and will do more damage than good. We always want to be moving our injuries —albeit non-painfully — because that helps to start to loosen up tight muscles, get the blood flowing to the area, etc.
When you stub your toe or hurt your finger the first thing you do is move and take it to its full range of motion as possible. As long as it does not hurt more the movement and other rubbing that we do helps o tell our nervous systems that everything is relatively fine and it does not need to impose any restrictions on movement or dial up our pain sensations to prohibit us from potentially damaging the tissues more.
However, we are taught that we generally should not be moving other injuries and it is definitely detrimental to our overall health. Do not get me wrong there is some times where movement restriction is necessary such as after surgery where delicate tissues need to heal. Likewise, if the pain is made worse by movement and a doctor should be checking you out then this may be another instance where pure rest indicated. These are cases are more rare and you will tend to know when these cases present themselves because you will probably be going to the emergency room or doctor immediately.
Regardless, if I were to put a number on it I would say that movement and/or exercise in general should be used in healing about 90-95% of injuries. Ice, heat, anti-inflammatories, ultrasound, e-stim, etc.
are all well and good, but most of the time they are not needed (or can be used in the context of helping speeding healing in some cases).
Tdo not think I have to elaborate on why pushing through pain is a bad idea. Our bodies have pain to tell us when we are damaging things. If you want to make an injury worse the best thing to do is push through pain. There are some exceptions, but generally they should only be done under a qualified medical professional or physical therapist during rehabilitation.
If you are having issues is pain soft tissue work and non-painful mobility work is extremely important. One of the major factors in eliminating pain is the gate control theory of pain. The gate control theory of pain shows us how to help dull down the pain so the body can heal itself better.
Al of the fibers under *gate control" are sensory afferents from the skin, muscles, ligaments, and joints. The large fibers specifically are the ones that travel fastest — alpha and beta fibers (Ia and II, and Ib respectively) — in humans these are golgi tendon organs and muscle spindles. The small fibers tend to be smaller afferents responsible for nociceptive (pain) input including Adelta and C fibers.
The theory goes that stimulation of the large alpha and beta fibers can interfere and help dull the body’s sense of pain from the smaller delta and C fibers. What stimulates alpha and beta fibers? That’s right: soft tissue work and movement.
Many people have probably experienced this phenomena but did not know it. Have you ever injured yourself during exercise? For instance, possibly a skinned shin during a deadlift or clean and jerk? Or you were running and hit a limb or toe on something but it did not hurt? Or been so hyped up for something that you did not feel the pain such as in a fight or flight situation?
Since there is so much feedback from the faster fibers from movement and/or exercise or total body sympathetic response it literally drowns out the pain fiber sensations that are sent to the brain. And you do not feel any pain.
The gate control theory of pain has been expounded upon in the recent decade to give way to the neuromatrix theory of pain. Basically, since all pain is in the brain, a theory must be able to explain phantom pain. Therefore, it must take into account how we perceive a nociceptive (pain) stimulus and how it may relate to cases where there is pain but no nociceptive input but pain is present.
The neuromatrix theory of pain focuses on somatosensory input (which includes all of the gate control theory above), the limbic system (emotion, behavior, memory, and smell), and thalamocortical systems (processing of these inputs).
Thus, if pain especially chronic type of pain, is imprinted strongly enough on our system (c.g. a neurosignature), a stimulus that does not cause pain may be interpreted in the brain as pain. This would cause phantom pain, or pain where there is no tissue damages. This is typical of extensive chronic pain which we will discuss a bit later.
How much is too much?
Generally, movement is good as long as the pain, inflammation, swelling, are improving or at least staying neutral. Most of the time if you are focused on movement or mobilizing a joint you should end up feeling better than when you started
This is important for any stretching, mobility, or prehabilitation work as well.
Acute injuries are a difficult topic to discuss directly which is why you should always talk to your physical therapist about rehabilitation progression and planning.
It is important not to progress too fast as it lear that injured tissues are vulnerable to reinjury more than healthy tissues. However, it is important not to baby injuries such that they lead to functional impairments to compensations that interfere with normal activities or sports,
Any questions during the rehabilitative phase should be addressed to the appropriate health care professional. If they cannot answer your questions then you may want to search for a new one. Although it depends" may not be the answer you're looking for which is often the case, but most health professionals if they are good should be able to give you a decent time frame or progressive plan or alternatives if you ask.
Chronic pain also presents an interesting case. After about 3-4+ months most of the damage from injuries are healed. While there may be some restrictions in movement via things such as scar tissue, if there is chronic pain present without damage to the soft tissues why is it still there?
The answer lics in our nervous systems. Our brains can interpret stimuli any way it wants and there are a lot of disorders such as aphasias where our brains incorrectly process what we hear and how we understand and speak out our response. The same is true of chronic pain after injuries.
When it all comes down to it and we have chronic pain after 6 months and it continues we can almost always know that our brains are interpreting almost any sensation or movement that gives feedback to the nervous system as pain.
There are many keys to rehabbing chronic pain, but I think the best approach is the graded response which can be approached from two direetions. First, the *fear" response (or phobia) psychology where people are gradually introduced to things they fear such as spiders and is continually progressed such that they eventually see that they really have nothing to fear of that. This can be introduced with proper
gradation in movements starting from simple movements building up to more complex or greater movements.
The second approach is through somatosensory experience. If we take people through a variety of sensory experiences even near painful and demonstrate that on normal tissues the same near pain or pain response is not normal we can start to get the brain to realize that it is incorrectly interpreting these responses. After all, if someone thinks that even placing a hand on a painful area is going to hurt are they not going to tense up all their muscles and have a fear avoidance reaction of trying to move out of the way at all costs? The key is to introduce the sensory experiences gradually just like with exercise such that we limit the fear/pain/sympathetic responses and help restore proper activity within the nervous system.
I think that both of these techniques (and there are probably others that I do not have time to cover) are very useful in understanding that our bodies are not just based on musculoskeletal factors. We need to understand that movements and developing mobility is actually a combination of neuromuscular and musculoskeletal factors including even some primary neurological factors as well
After all we know that some people even with hours of stretching can never get any flexibility. Why?
Muscle spindles (gamma motor neurons) govem a muscle’s length. The nervous system controls these fibers. When they are "tightly wound" the muscle does not respond very well to length increases and stays tight,
This can happen for a variety of reasons but the most eluting is when you have spinal cord injury or stroke. When upper cerebral control is cut off from the spinal cord, the inhibion that the cerebral cortex puts on these gamma motor neurons is lost. Thus, they become overactive and the muscles tend to get extremely tight and hypertonic. You can this in the synergistic patterns where the a lot of the flexors tighten up and the arms, legs, and body start to move into the fetal position as they all sart to contract.
I made this point just to say that flexibility and mobility are not just about lengthening the muscles and connective tissues. We have to take into account how the nervous system responds to these exercises.
What to do?
Tough question.
Gate control theory tends to be variable, and delving into the neuromatrix theory of pain is a complex process. Sometimes the feedback from the muscle movement activates pain sensations when it should not with chronic pain. Sometimes it helps. If movement has pain, but does not increase it then it is generally best to move even if there is pain. It will get better as the body relearns how to sort out the sensations coming from its fibers,
Conditioning or graded response will also work. You have to take these things slowly and introduce the movement back. Preferably as stated before the small amounts of movements and mobility work will only have lower levels of pain or stiffness. However, as the body begins to lean again how to differentiate between them you can increase the movement,
It has been shown in studies that "chronic pain" is less in countries where there is no such thing as time off work or workers compensation. The mindset of the person is very critical to overcoming any type of chronic pain, so you really have to believe that you can do it along with the other protocols.
So in this section I am not going to talk about all of the possible prehabilitation, mobility, and flexibility exercises as books have been written on these topics already. However, what I am going to to is talk about the various exercises I think tend to help the most for all of these different areas of the body especially in the context of bodyweight training.
If you already have your own mobility or warm ups that work then by all means use those instead. You know your body better than I do. I do not have any particular preference for what is done as long as the exercises are helping you improve your abilities, performance, and stave off injuries,
This material should not be taken lightly because anyone that wants to seriously train strength whether it is bodyweight or weight training will know that injuries can easily sneak up on you. Thus, it pays to be proactive in attempting to avoid them rather than wait for them to occur and then rehabilitate: them.
Standard static stretching is one where you do anywhere from about is to even a couple of minutes. Typically a regimen of about 30-40s for about 3-5 sets has been shown to be optimal from the studies. For ach stretch I like to tell people that you want to get just a little bit further than you did the first time. The best way is to get them to relax, and the best way to do that is utilize some deep breathing techniques and let the muscles lengthen on the exhalation of breath. Utilizing a program such as yoga can also be effective.
I you are one of the people who is resistant to this type of stretching you will find out within a week or two of absolutely no gains from this type of stretching. Thercfore, we have to move on to more effective methods.
Proprioceptive neuromuscular facilitation is another method that tries to take aim at the nervous system to relax the muscle. There are a lot of techniques that fall under the PNF umbrella, but by far the most common are the hold/relax and contract/relax methods. In these techniques, the person being stretehed will contract or hold against another person for a set amount of time. After that the muscle is lengthened and allowed to relax for another set amount of time. This helps to relax the muscle spindles at the edge of the range of motion which may help people who are chronically tigh.
Typically, about 2-5 cycles of hold/relax or contract/relax are effective. The hold and contract phases can be anywhere from about 5-15s depending on how tight the muscles are. Remember, you have to fatigue the muscle to allow it to start releasing from its shortened length. I typically like about 5-10s. The
relax phase can be anywhere from about 10-30s. I like about 10-13s for this phase. All in all, with a contract phase of 10s and a relax phase of 155 the total stretching time ends up being about 80s total.
Another variation off of this is to contract the opposing muscles during the relax phase. This means that if you were stretching the hamstrings then you can contract the hip flexors and quadriceps in the relax phase where the hamstrings are lengthening. This goes off of the principle of reciprocal inhibition in which the body naturally will relax the muscles on the opposite side of the joint(s) as one muscle is activated. This can be particularly effective for those who are extremely tight,
Another method that may help is tilizing the patellar reflexive arc to inhibit the hamstrings. The way to perform this would be to hit the patellar tendon like the doctor does to check your reflexes. Hit it multiple times and allow the reflexive arc to active and inhibit the hamstrings. Then do the PNF type of stretching. I have used this fairly successful to some degree in very tight people.
Full range of motion movements taken to the edge of the range of motion have been shown in the studies to be more effective than static stretching. For example, if you are performing weighted squats you will want to descend to the bottom of the squat as far as possible until you feel a stretch on the hamstrings If you continue to perform squats this way you will naturally increase your range of motion, especially as the weights get heavier.
Another way to implement this is the "asian squat." Get into the bottom position of the squat and then shift the weight all around on the feet to stretch out the calves, hamstrings, glutes, quads, back, ctc. For those who are extremely tight hanging out in the bottom position for even up to 5 minutes or more can be more effective than even PNF type stretching.
Remember, the only way to gain range of motion is to move to the edges of your range of motion and allow the body to accommodate to the length increases. You cannot improve flexibility or mobility without doing this.
Mobility is typically coupled with the full range of motion movements. The movements can be smaller in nature although they both work nearer towards the edge of range of motion to increase proficiency there,
Let us first talk about the hips. Many of gymnastics type progressions for bodyweight training such as the press handstands focus on general hip mobility. Therefore, most of the problems cropping up with the hips will be focused on issues regarding improving the type of mobility that is needed in the hips. Issues such as like cramping, possibly impingement, and strains are the common ones that crop up.
If general strength for the legs is based on weighted work such as deadlifts and squats that i great. Ideally, this would lead to the development of deep squats which are a fundamental human movement. This would decrease the amount of work we have to work on hip mobility.
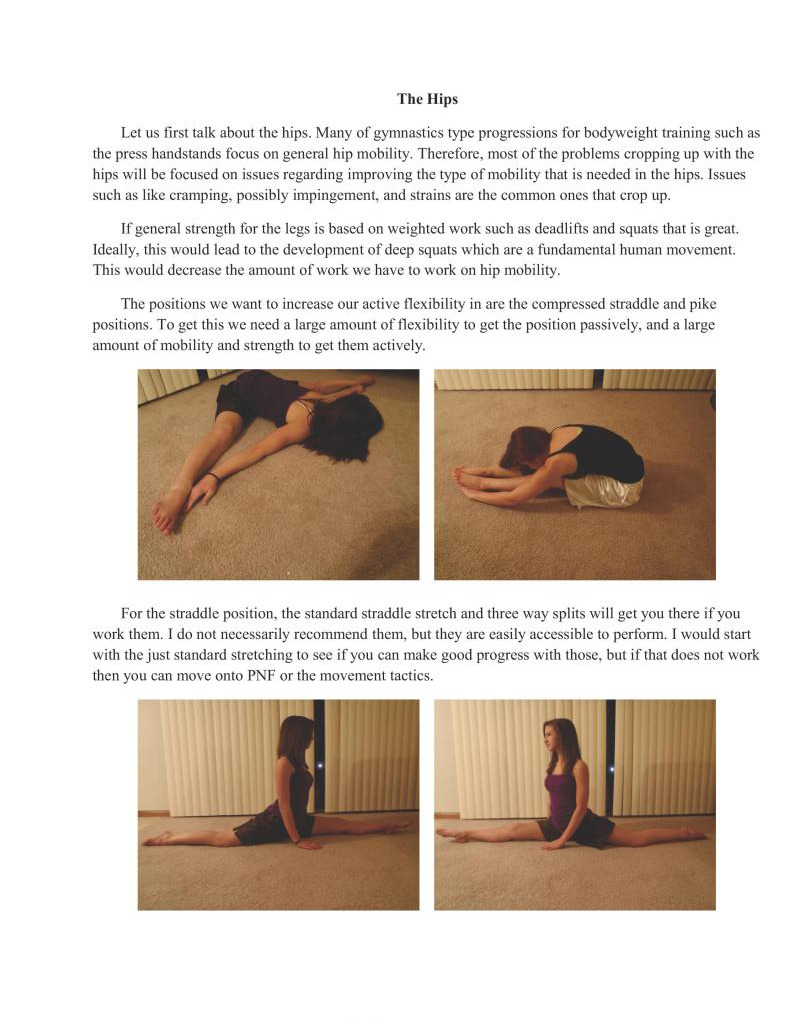
The positions we want to increase our active flexibility in are the compressed straddle and pike positions. To get this we need a large amount of flexibility to get the position passively, and a large amount of mobility and strength to get them actively.
For the straddle position, the standard straddle stretch and three way splits will get you there if you work them. I do not necessarily recommend them, but they are easily accessible to perform. I would start with the just standard stretching to see if you can make good progress with those, but if that does not work then you can move onto PNF or the movement tactics.
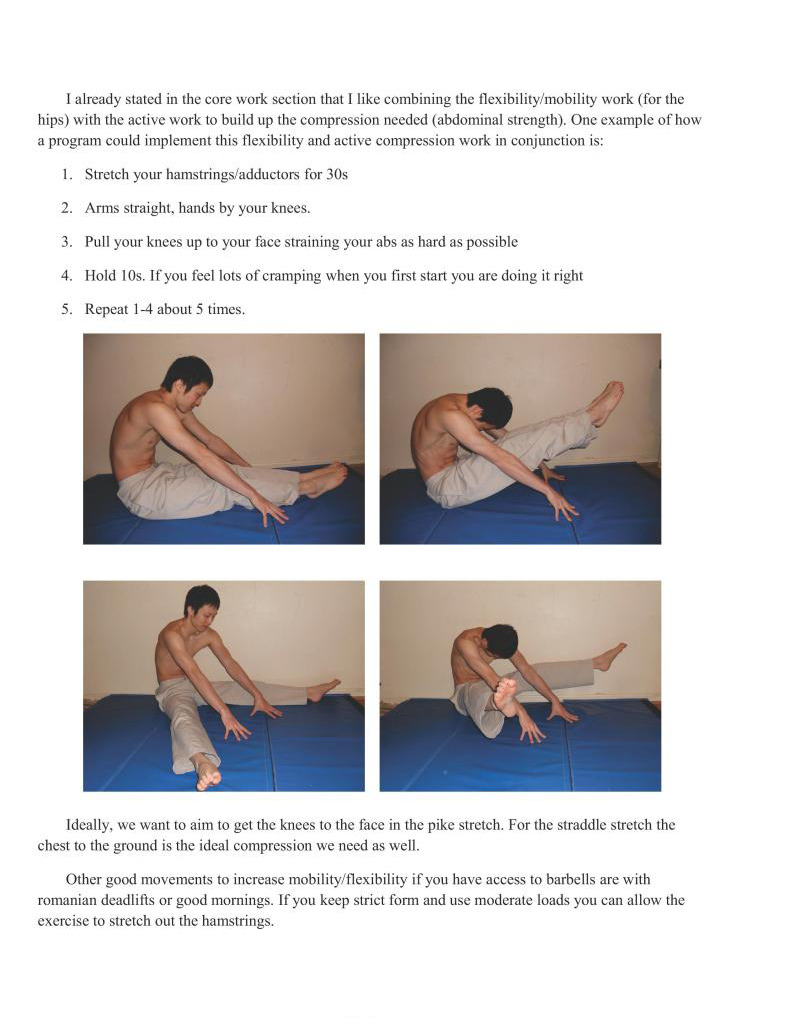
Talready stated in the core work section that I like combining the flexibility/mobility work (for the hips) with the active work to build up the compression needed (abdominal strength). One example of how a program could implement this flexibility and active compression work in conjunction is:
Ideally, we want to aim to get the knees to the face in the pike stretch. For the straddle stretch the chest to the ground is the ideal compression we need as well
Other good movements to increase mobility/flexibility if you have access to barbells are with romanian deadlifts or good mornings. If you keep strict form and use moderate loads you can allow the exercise to stretch out the hamstrings
Closed chain exercises where the feet are in contact with the ground are particularly effective. Another couple bodyweight exercises that can be used are from the lunge position.
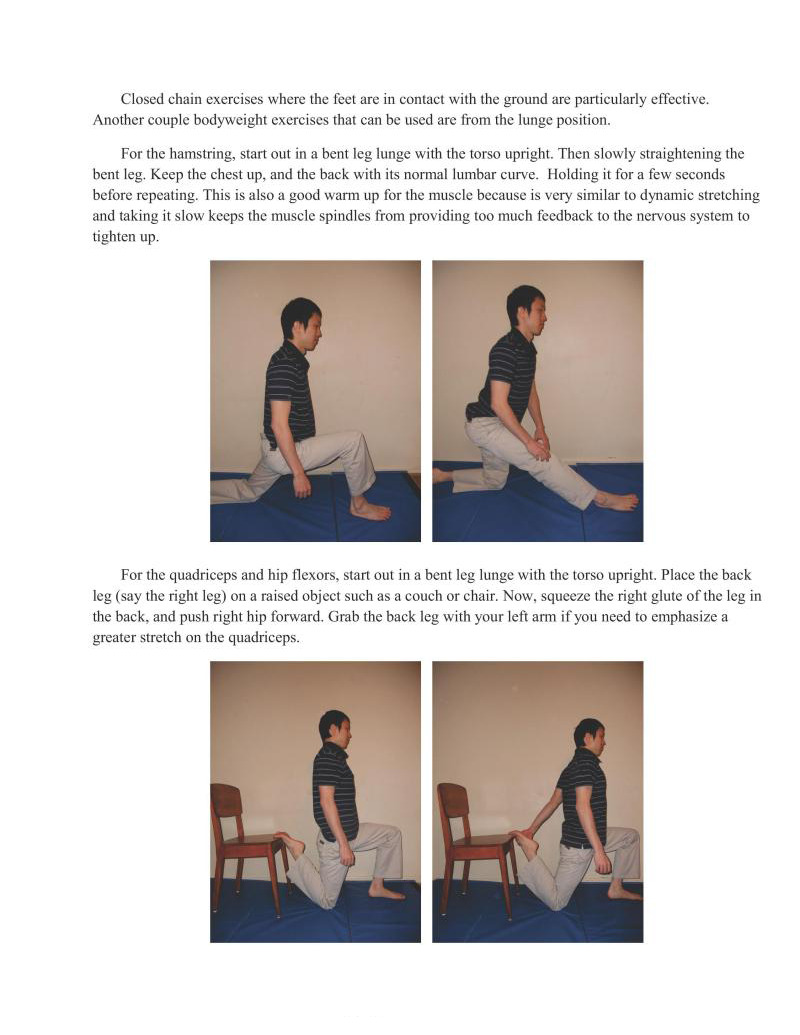
For the hamstring, start out in a bent leg lunge with the torso upright. Then slowly straightening the bent leg. Keep the chest up, and the back with its normal lumbar curve. Holding it for a few seconds before repeating. This is also a good warm up for the muscle because is very similar to dynamic stretching and taking it slow keeps the muscle spindles from providing too much feedback to the nervous system to tighten up.
For the quadriceps and hip flexors, start out in a bent leg lunge with the torso upright. Place the back leg (say the right leg) on a raised object such as a couch or chair. Now, squeeze the right glute of the leg in the back, and push right hip forward. Grab the back leg with your left arm if you need to emphasize a greater stretch on the quadriceps.
We are not going to discuss the cervical vertebrae beyond this paragraph. The only thing you need to know is to keep them neutral during any techniques described in this book. Craning the neck during any skills can impinge on the nerves coming out of the neck and that may decrease force output during strength work or lead to improper movement pattens in skill work. Avoid distorting cervical vertebrac mechanics if at al possible.
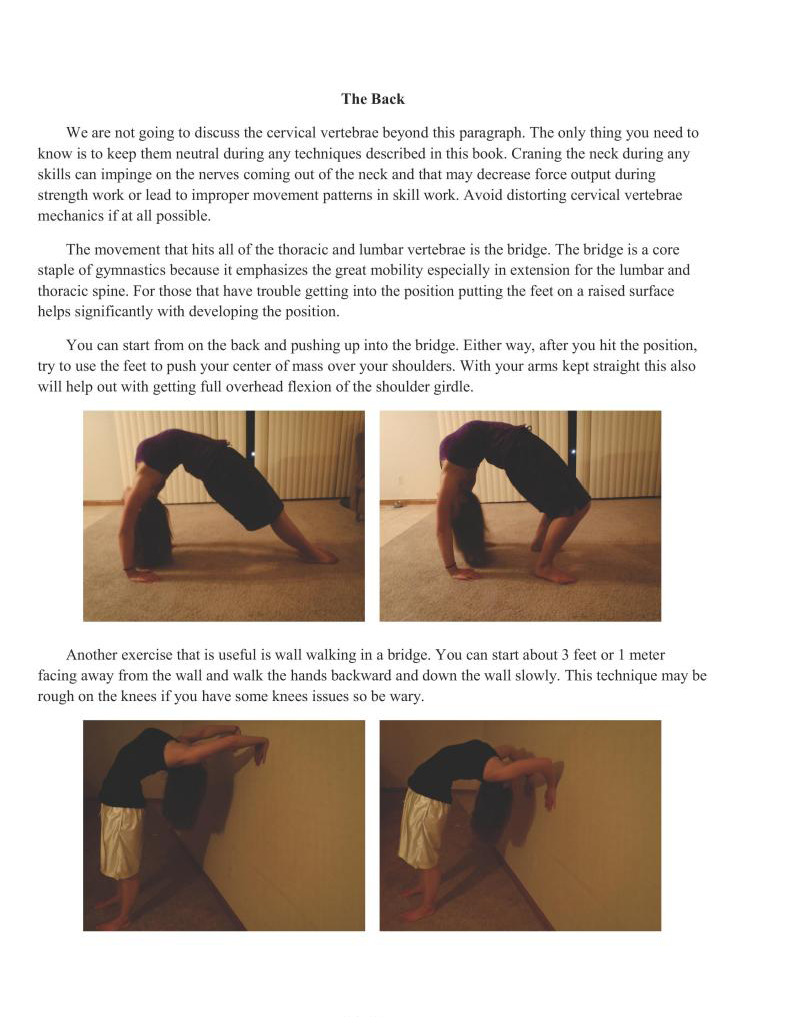
The movement that hits all of the thoracic and lumbar vertebrac is the bridge. The bridge is a core staple of gymnastics because it emphasizes the great mobility especially in extension for the lumbar and thoracic spine. For those that have trouble getting into the position putting the feet on a raised surface helps significantly with developing the position.
You can start from on the back and pushing up into the bridge. Either way, after you hit the position, ry to use the feet to push your center of mass over your shoulders. With your arms kept straight this also will help out with getting full overhead flexion of the shoulder girdle.
Another exercise that is useful is wall walking in a bridge. You can start about 3 feet or 1 meter facing away from the wall and walk the hands backward and down the wall slowly. This technique may be rough on the knees if you have some knees issues so be wary.
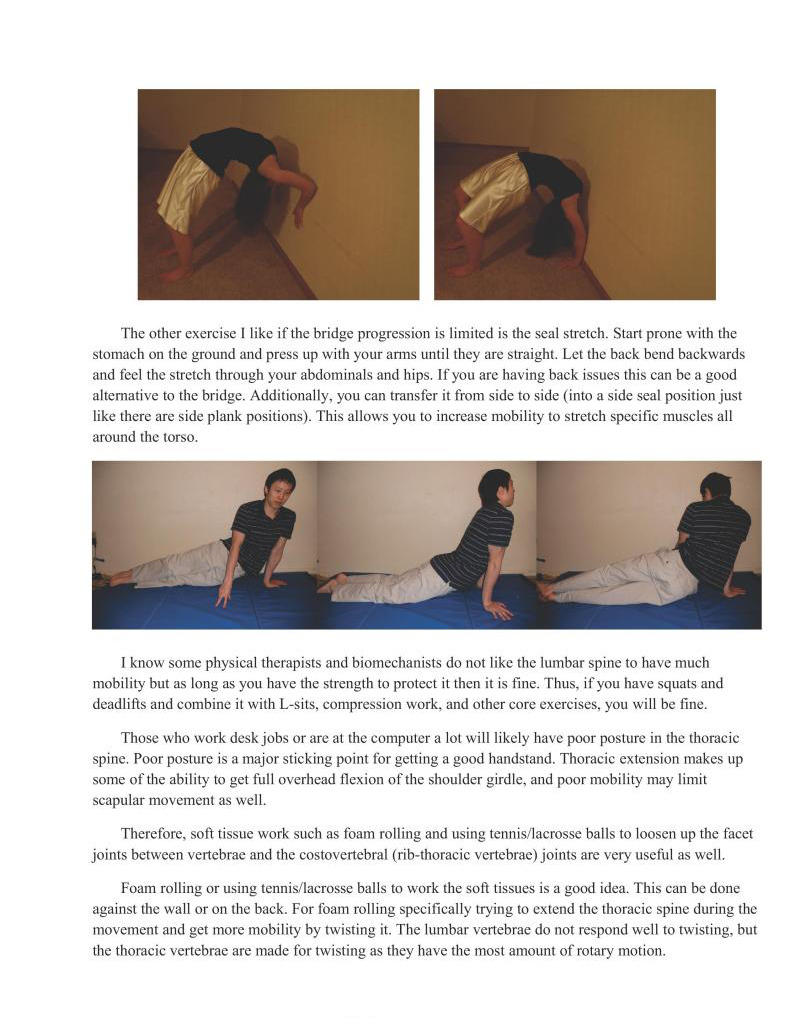
The other exercise | like if the bridge progression is limited is the seal stretch. Start prone with the stomach on the ground and press up with your arms until they are straight. Let the back bend backwards and feel the stretch through your abdominals and hips. If you are having back issues this can be a good aliemative to the bridge. Additionally, you can transfer it from side to side (into a side seal position just like there are side plank positions). This allows you to increase mobity to stretch specific muscles all around the torso.
I know some physical therapists and biomechanists do not like the lumbar spine to have much mobility but as long as you have the strength to protect it then it is fine. Thus, if you have squats and deadlifts and combine it with L-sits, compression work, and other core exercises, you will be fine.
Those who work desk jobs or are at the computer a lot will likely have poor posture in the thoracic spine. Poor posture is a major sticking point for getting a good handstand. Thoracic extension makes up some of the ability to get full overhead flexion of the shoulder girdle, and poor mobility may limit scapular movement as well.
Therefore, soft tissue work such as foam rolling and using tennis/lacrosse balls to loosen up the facet joints between vertebrae and the costovertebral (rib-thoracic vertebrae) joints are very useful as well
Foam rolling or using tennis/lacrosse balls to work the soft tissues is a good idea. This can be done against the wall or on the back. For foam rolling specifically trying to extend the thoracic spine during the movement and get more mobility by twisting it. The lumbar vertebrae do not respond well to twisting, but the thoracic vertebrae are made for twisting as they have the most amount of rotary motion.
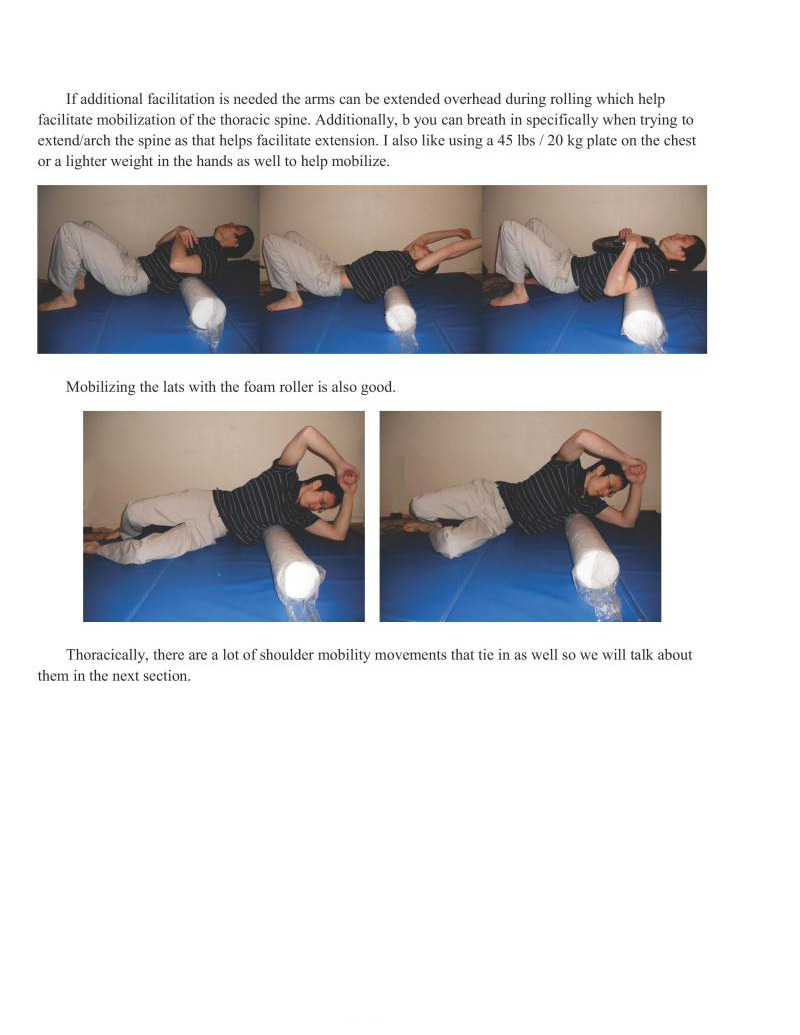
If additional facilitation is needed the arms can be extended overhead during rolling which help facilitate mobilization of the thoracic spine. Additionally, b you can breath in specifically when trying to extend/arch the spine as that helps facilitate extension. I also like using a 45 lbs / 20 kg plate on the chest ora lighter weight in the hands as well to help mobilize.
Mobilizing the
Thoracically, there are a lot of shoulder mobility movements that tie in as well so we will talk about them in the next section.
I spent a large amount of time in chapters 1 and 4 talking about how the shoulder is the lynchpin of the upper body and also the most mobile. This means that it has a relatively greater potential for injury at the joint. This is why we need to take care of it.
Take the manna and horizontal pulling specifically to balance out much of the pressing and vertical pulling work. However, sometimes that is not enough and shoulder issues may develop beyond that which is why this section needs to be written.
Some of the more isolation exercises that are extremely good in bringing up posterior shoulder strength and correcting some of the imbalances are the LYTPs. LYTPs in particular hit the thomboids, middle and lower traps, posterior scapular muscles, and other deeper posterior structures which are neglected. Additionally, lower trapezius work specifically (in the Y movement) is very useful for building
the strength and musculature for the straight arm presses.
All of these movements are performed lying prone on the table. Al of these exercises can be performed with unweighted, with dumbbells, or any kind of makeshift weights.
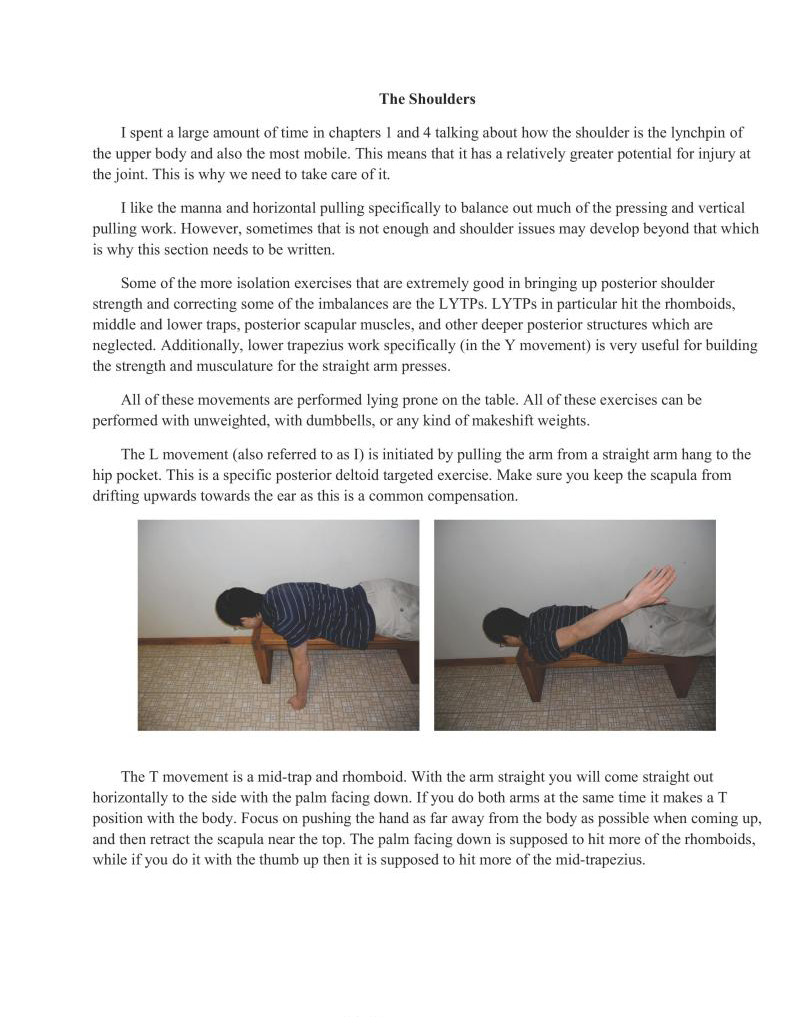
The L movement (also referred to as 1) is initiated by pulling the arm from a straight arm hang to the hip pocket. This is a specific posterior deltoid targeted exercise. Make sure you keep the scapula from drifting upwards towards the car as this is a common compensation.
The I movement is a mid-trap and rhomboid. With the arm straight you will come straight out horizontally to the side with the palm facing down. If you do both arms at the same time it makes a T position with the body. Focus on pushing the hand as far away from the body as possible when coming up, and then retract the scapula near the top. The palm facing down is supposed to hit more of the thomboids, while if you do it with the thumb up then it is supposed to hit more of the mid-trapezius.
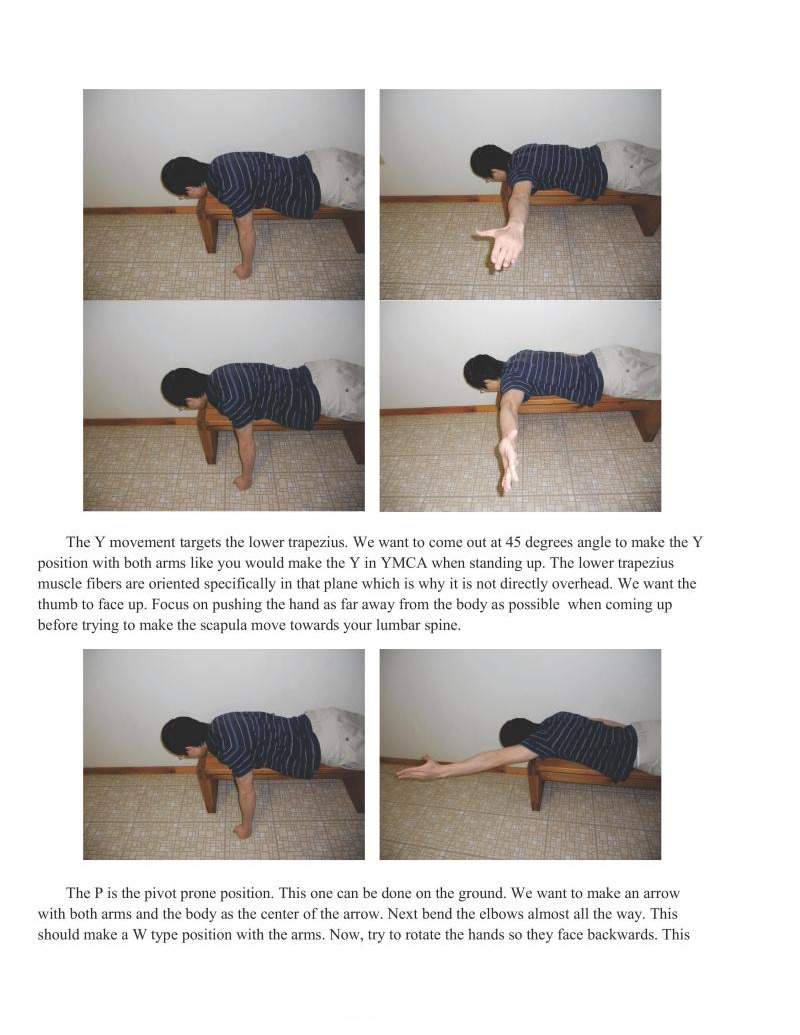
The Y movement targets the lower trapezius. We want to come out at 45 degrees angle to make the Y position with both arms like you would make the Y in YMCA when standing up. The lower trapezius muscle fibers are oriented specifically in that plane which is why it is not directly overhead. We want the thumb to face up. Focus on pushing the hand as far away from the body as possible when coming up before trying to make the scapula move towards your lumbar spine.
The P is the pivot prone position. This one can be done on the ground. We want to make an arrow with both arms and the body as the center of the arrow. Next bend the elbows almost all the way. This should make a W type position with the arms. Now, try to rotate the hands so they face backwards. This
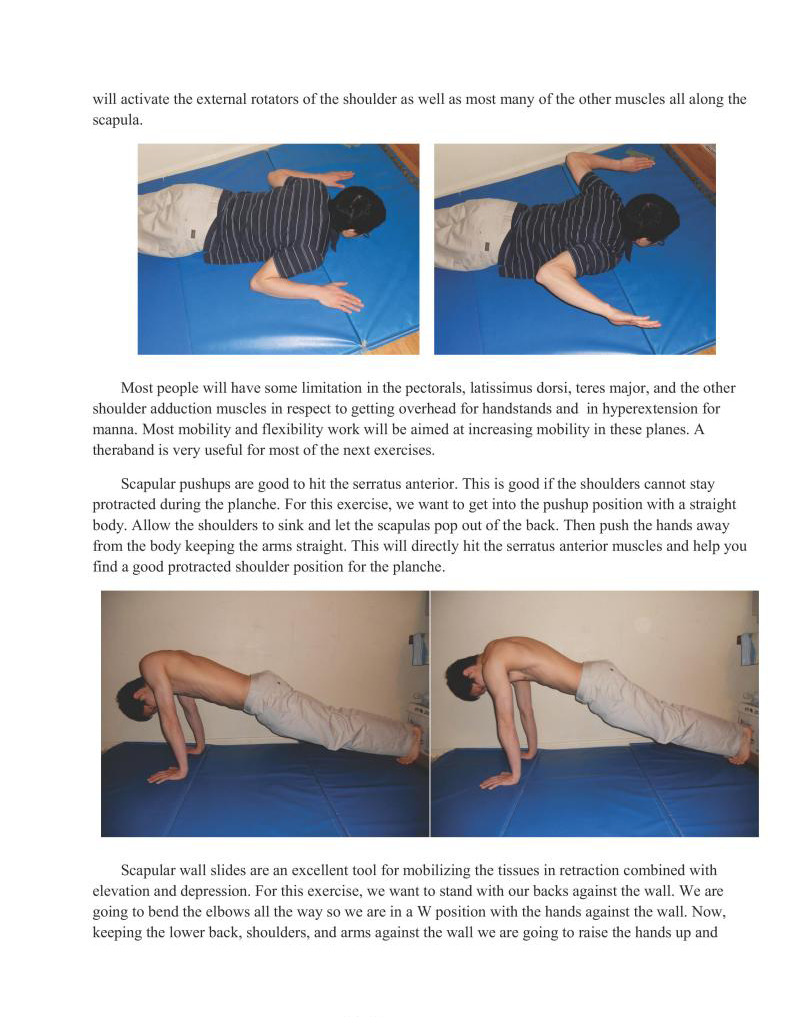
will activate the external rotators of the shoulder is well as most many of the other muscles all along the scapula
Most people will have some limitation in the pectorals, latissimus dorsi, teres major, and the oth shoulder adduction muscles in respect to getting overhead for handstands and. in hyperextension for manna. Most mobility and flexibility work will be aimed at increasing mobility in these planes. A theraband is very useful for most of the next exercises.
Scapular pushups are good to hit the serratus anterior. This is good if the shoulders cannot stay protracted during the planche. For this exercise, we want to get into the pushup position with a straight body. Allow the shoulders to sink and let the scapulas pop out of the back. Then push the hands away from the body keeping the arms straight, This will directly hit the serratus anterior muscles and help you find a good protracted shoulder position for the planche.
Scapular wall slides are an excellent tool for mobilizing the tissues in retraction combined with
elevation and depression. For this exercise, we want to stand with our backs against the wall. We are going to bend the elbows all the way so we are in a W position with the hands against the wall. Now, keeping the lower back, shoulders, and arms against the wall we are going to raisc the hands up and
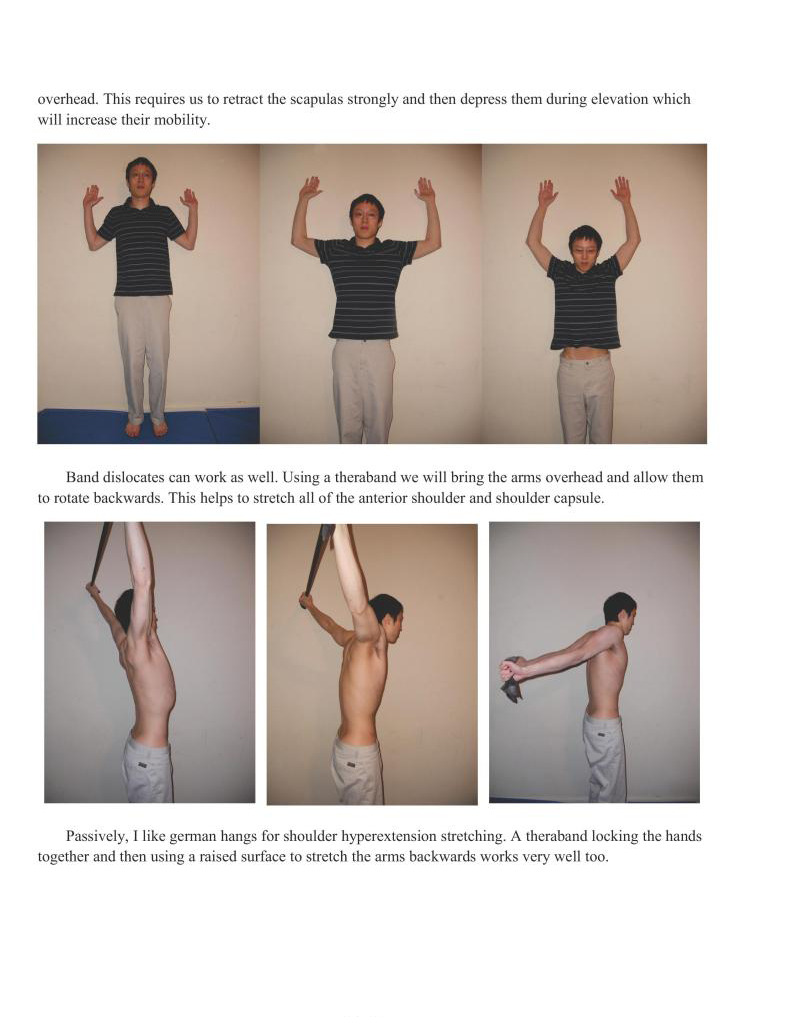
overhead. This requires us to retract the scapulas strongly and then depress them during elevation which will increase their mobility.
Band dislocates can work as well. Using a theraband we will bring the arms overhead and allow them to rotate backwards. This helps to stretch all of the anterior shoulder and shoulder capsule.
Passively, I like german hangs for shoulder hyperextension stretching. A theraband locking the hands together and then using a raised surface to stretch the arms backwards works very well too.
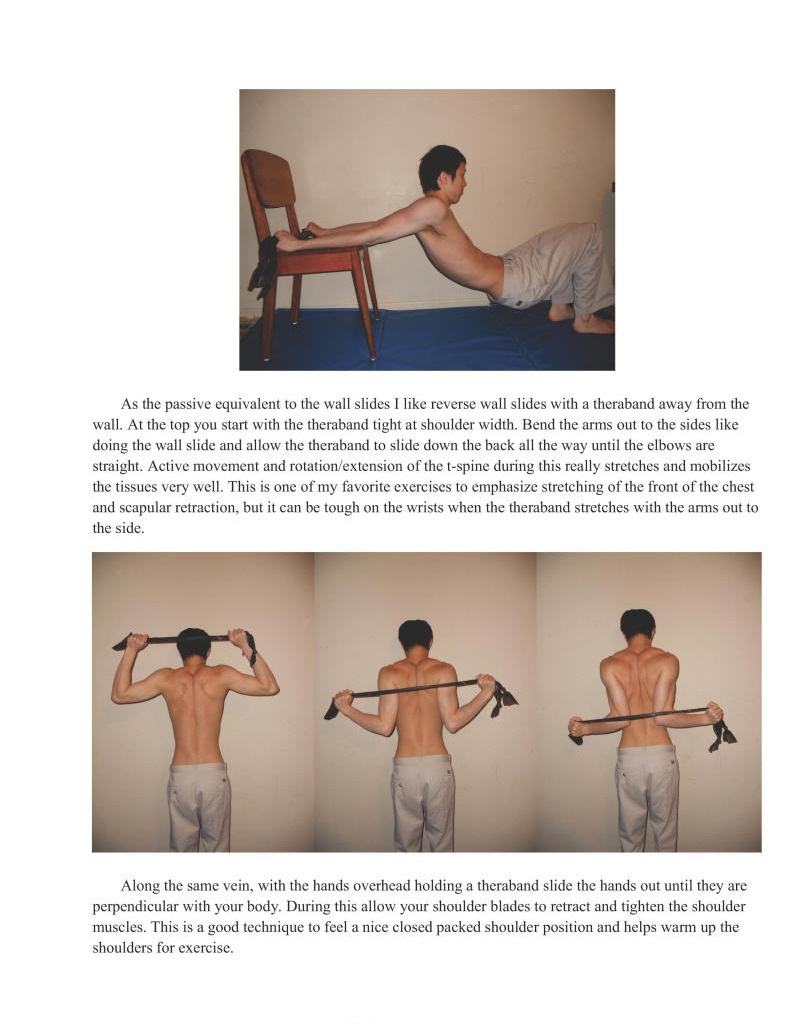
As the passive equivalent to the wall slides 1 like reverse wall slides with a theraband away from the wall. At the top you start with the theraband tight at shoulder width. Bend the arms out to the sides like doing the wall slide and allow the theraband to slide down the back all the way until the elbows are straight. Active movement and rotation/extension of the t-spine during this really stretches and mobilizes the tissues very well. This is one of my favorite exercises to emphasize stretching of the front of the chest and scapular retraction, but it can be tough on the wrists when the theraband stretches with the arms out to the side.
Along the same vein, with the hands overhead holding a theraband slide the hands out until they are perpendicular with your body. During this allow your shoulder blades to retract and tighten the shoulder muscles. This is a good technique to feel a nice closed packed shoulder position and helps warm up the shoulders for exercise.
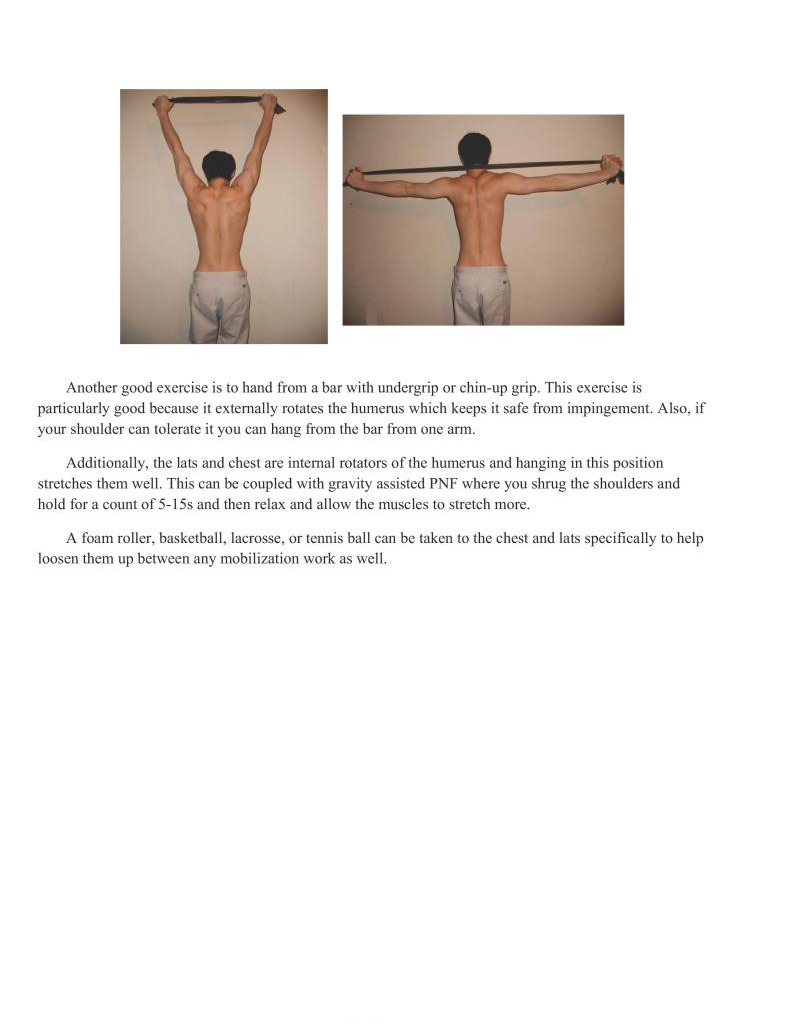
Another good exercise is to hand from a bar with undergrip or chin-up grip. This exercise is particularly good because it extemally rotates the humerus which keeps it safe from impingement. Also, if your shoulder can tolerate it you can hang from the bar from one arm.
Additionally, the lats and chest are intemal rotators of the humerus and hanging in this position stretches them well. This can be coupled with gravity assisted PNF where you shrug the shoulders and hold for a count of 5-15 and then relax and allow the muscles to stretch more.
A foam roller, basketball, lacrosse, or tennis ball can be taken to the chest and lats specifically to help loosen them up between any mobilization work as well.
The elbows are a relatively simple joint which does not need to be discussed that much as far as mobility and flexibility are concerned. However, it is particular vulnerable to injuries so proper prehabilitation is important.
In most cases the biggest issues tend to be tendonitis or overuse stress to the joints. Rings in particular s very tough on the elbows, and the upper level pulling moves such as one arm chin-ups and ron cross are tough on the joints.
There are a lot of muscles that insert around the elbow both from the arm and forearm which often can get gummed up putting additional pressure on the joints and tendons. Thus, it is important to keep these tissues healthy.
Besides tendonitis protocol for a specific pathological state, massage to the tissues to loosen them up both in the bent and straight arm position.
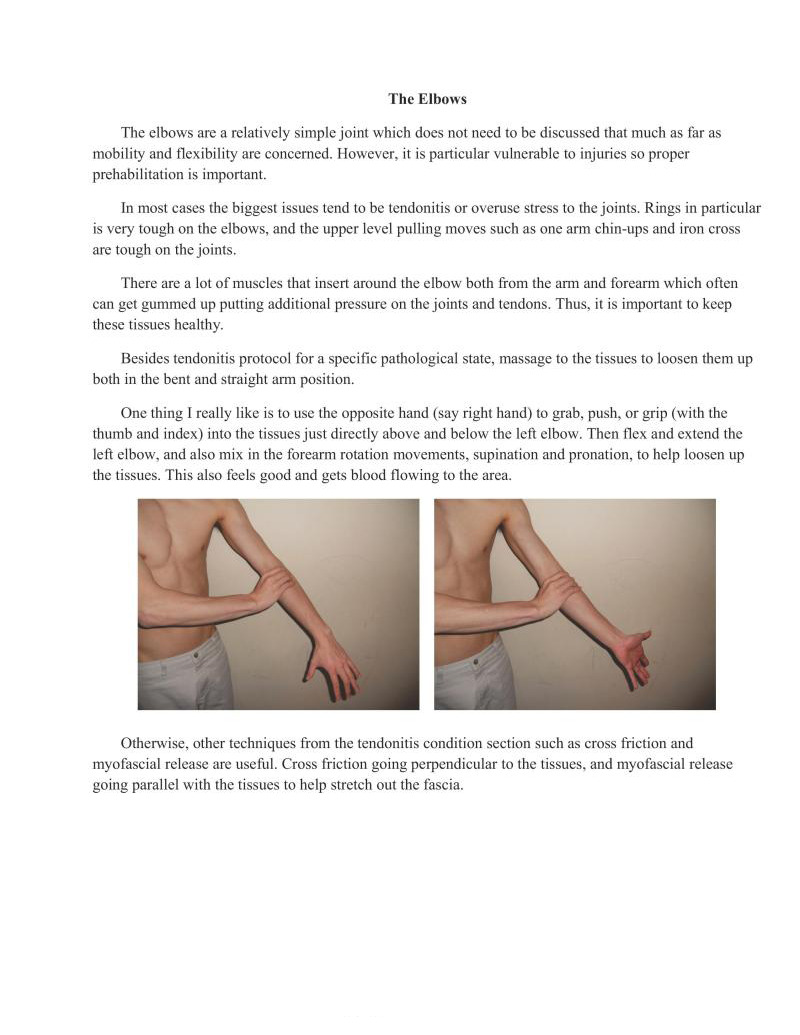
One thing I really like is to use the opposite hand (say right hand) to grab, push, or grip (with the thumb and index) into the tissues just directly above and below the left elbow. Then flex and extend the left elbow, and also mix in the forearm rotation movements, supination and pronation, to help loosen up the tissues. This also feels good and gets blood flowing to the area.
Otherwise, other techniques from the tendonitis condition section such as cross friction and myofascial release are useful. Cross friction going perpendicular to the tissues, and myofascial release going parallel with the tissues to help streteh out the fascia.
The wrists are an interesting joint namely because of their use.
Wrist pushups are certainly a good exercise in terms of mobility and prehabilitation, but I have seen them taken to almost magical status.
Wrist pushups take the wrist through a full range of motion with the wrist in flexion, which is the unused movement of the wrist. This alone makes it good because it helps to balance out the forearm extensors and flexors of the wrist. Additionally, it strengthens the extensors and stretches them as they are traditionally weak and tight from the wrists being in flexion and gripping a lot of the time.
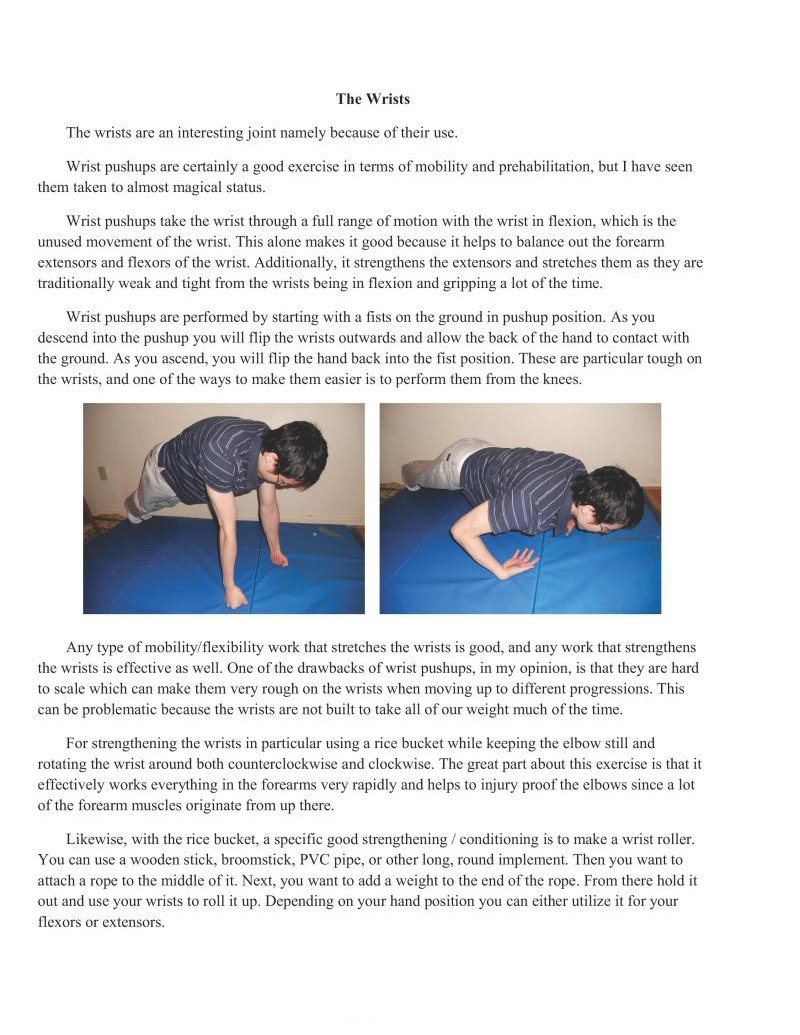
Wrist pushups are performed by starting with a fists on the ground in pushup position. As you descend into the pushup you will lip the wrists outwards and allow the back of the hand to contact with the ground. As you ascend, you will flip the hand back into the fist position. These are particular tough on the wrists, and one of the ways to make them easier is to perform them from the knees.
Any type of mobility/flexibility work that stretches the wrists is good, and any work that strengthens the wrists is effective as well. One of the drawbacks of wrist pushups, in my opinion, is that they are hard 10 scale which can make them very rough on the wrists when moving up to different progressions. This can be problematic because the wrists are not built to take all of our weight much of the time.
For strengthening the wrists in particular using a rice bucket while keeping the elbow still and rotating the wrist around both counterclockwise and clockwise. The great part about this exercise is that it
effectively works everything in the forearms very rapidly and helps to injury proof the elbows since a lot of the forearm muscles originate from up there.
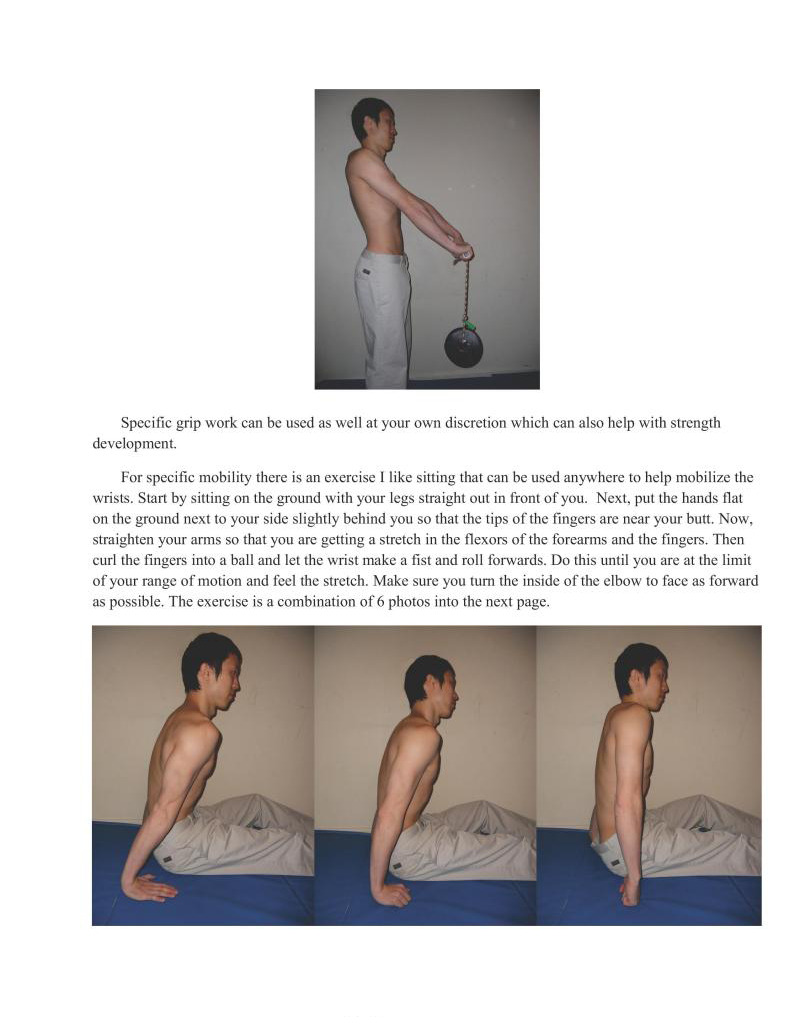
ikewise, with the rice bucket, a specific good strengthening / conditioning is to make a wrist roller. You can use a wooden stick, broomstick, PVC pipe, or other long, round implement. Then you want to attach a rope to the middle of it. Next, you want to add a weight to the end of the rope. From there hold it out and use your wrists to roll it up. Depending on your hand position you can either utilize it for your flexors or extensors.
Specific grip work can be used as well at your own discretion which can also help with strength development.
For specific mobility there is an exercise I like sitting that can be used anywhere to help mobilize the wrists. Start by sitting on the ground with your legs straight out in front of you. Next, put the hands flat on the ground next to your side slightly behind you so that the tips of the fingers are near your butt. Now, straighten your arms so that you are getting a stretch in the flexors of the forearms and the fingers. Then curl the fingers into a ball and let the wrist make a fist and roll forwards. Do this until you are at the limit of your range of motion and feel the stretch. Make sure you turn the inside of the elbow to face as forward as possible. The exercise is a combination of 6 photos into the next page.
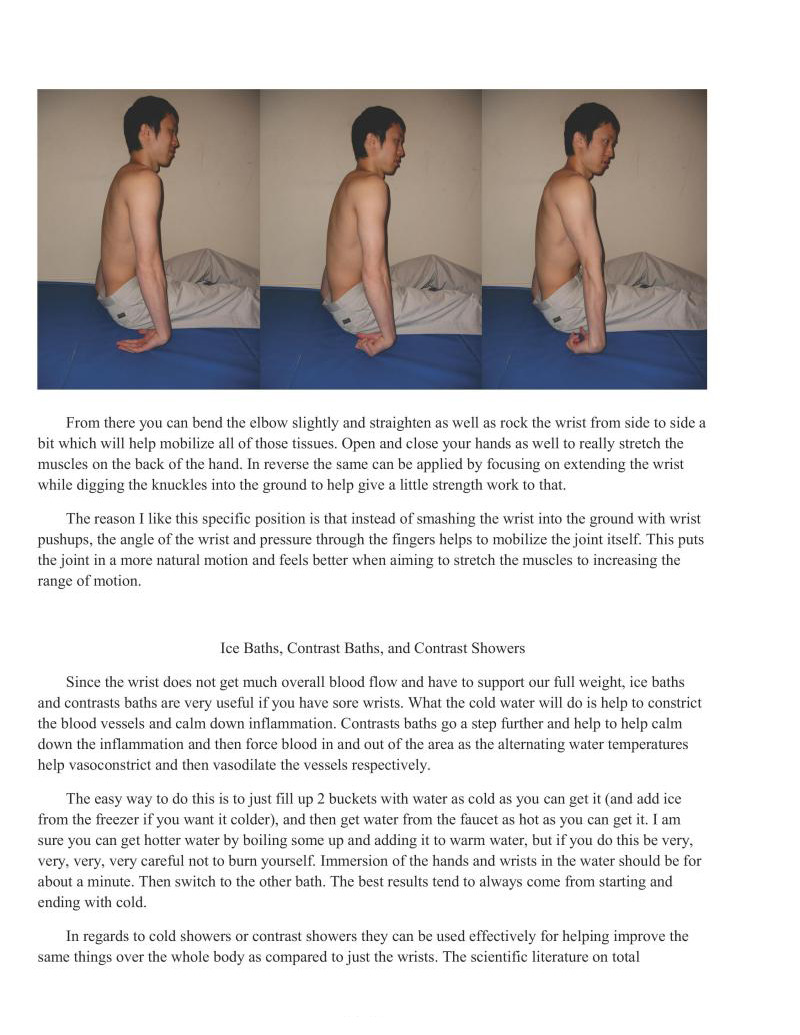
From there you can bend the elbow slightly and straighten as well as rock the wrist from side to side a bit which will help mobilize all of those tissues. Open and close your hands as well to really stretch the muscles on the back of the hand. In reverse the same can be applied by focusing on extending the wrist while digging the knuckles into the ground to help give a little strength work to that
The reason I like this specific position is that instead of smashing the wrist into the ground with wrist pushups, the angle of the wrist and pressure through the fingers helps to mobilize the joint itself. This puts the joint in a more natural motion and feels better when aiming to stretch the muscles to increasing the range of motion.
Since the wrist does not get much overall blood flow and have to support our full weight, ice baths and contrasts baths are very useful if you have sore wrists. What the cold water will do is help to constrict the blood vessels and calm down inflammation. Contrasts baths go a step further and help to help calm down the inflammation and then force blood in and out of the area as the alternating water temperatures help vasoconstrict and then vasodilate the vessels respectively.
The easy way to do this is to just fill up 2 buckets with water as cold as you can get it (and add ice from the freezer if you want it colder), and then get water from the faucet as hot as you can getit. | am sure you can get hotter water by boiling some up and adding it to warm water, but if you do this be very, very, very, very careful not to burn yourself, Immersion of the hands and wrists in the water should be for about a minute. Then switch to the other bath, The best results tend to always come from starting and ending with cold.
In regards to cold showers or contrast showers they can be used effectively for helping improve the same things over the whole body as compared to just the wrists. The seientific literature on total immersion ice baths and showers is conflicted. Most studies tend to show no benefit to these protocols in regard to soreness, improved performance, etc. However, my generalized take on this is that if it helps you, even if it is just psychological or placebo effective, then why not? I still continue to use them myself because they do seem to apply some minor benefits in regard to tissue health and quality.
The same concept for the wrist baths applies to the shower. Always start with cold and end with cold. It is not very fun, but when you get used to them it will be refreshing.
Calluses can be a huge problem if they get too big and rip. What I like to do is when they get too big is 10 take a nice long, hot shower. Then when they start to get white you can scratch them off fairly easily.
Another alternative is to soak them in a bucket with warm water much like the wrists. Once they get Soft and white you can scratch them off, or you can use a razor or knife to remove them.
Still yet another alternative is to take a nail clipper and clip them off. Whatever you choose to do b safe!
As for rips, they suck. You can get them anywhere in the hands. Generally, bodyweight training probably will not create any, but if you are training swinging movements or let them get too big or anything else that puts a lot of force on the hands it is possible to rips some of the skin.
For treating them I will start by using a nail clipper or scissors to remove the extra skin. You can rip them off with your hands, but you risk the chance that you rip more skin off. If you do decide to attempt to use this method you should definitely pull down and away. Pulling up will make the rip bigger, and pulling just horizontal does not put enough force on the skin to make it ip easier.
In regards to treating them when you training or at the gym 1 like to throw some chalk on them and get some work on it to stimulus mitogenesis (which is cell division which is needed to heal the wound). The only way you can actually rebuild the callus is to use the new skin. Go to pain tolerance, but do not go so much that you rip more or bleed. I also like putting salt on the wound and rubbing it in, but this is for the more masochistic of people who want their rips to heal faster.
However, when at home make sure you are stretching the hand out so that the new skin will be long enough such that when you open your hand all the way it will not tear a deeper hole in your hand. Likewise, moisturize at home so they do not crack which will also make them deeper.
This is akin to physical therapy where at therapy you are going to be working on rehabilitation. However, at home you are mostly going to take care of it and rest. Do not do anything fancy — the body is very good at healing itself if you take the right steps to allow it to heal. Sleep a lot, eat well, and let them heal
In this chapter we discussed how prehabilitation, mobility, and flexibility all related to each other in the context of keeping our bodies healthy.
We looked at some of the specifics on mobility and flexibility as to how they related to injury and pain. Applying techniques that utilize both the musculoskeletal and neuromuscular aspects represent the best way to overall target. everyone as some techniques do not work well for others. Acute and chronic pain will differ in the way it is treated.
Then we looked at some of the specific prehabilitation, mobility, and flexibility exercises and techniques that can be used in the five key areas utilized extensively in this book namely the hips, back, shoulders, elbows, and wrists.
We also discussed some of the finer points of contrast baths and showers, and we also looked at some information about rips and calluses.
Previous Chapter ... ... Next Chapter