Previous Chapter ... ... Next Chapter
This chapter specifically and this book in general are not meant to diagnose any injury. If you have an injury and are unsure, the best suggestion is to make an appointment with your doctor, physical therapist, or chiropractor and figure out what you are dealing with. At that point this chapter will be more useful.
Remember to keep in mind that these injuries will be discussed because they are common, but pain in the areas described does not immediately imply a specific injury even if it is a common injury. Take caution since exercises or rehabilitation techniques used for injuries which have not been diagnosed properly may actually worsen them. Have a qualified medical professional diagnose the condition.
Essentially, tendonitis is an overuse injury. There are many possible ways for it to develop such as muscle imbalances, scar tissue, general overuse, and/or under-recovery. Tendonitis develops because our connective tissues adapt and recor ‘Thus, heavy loads that can be handled by the muscles may not be able to be handled by connective tissues as you get stronger. Over time this has negative consequences, one of which is tendonitis.
struct slower than our muscles.
Tendonitis is characterized by three general stages.
The first stage is characterized by the *-itis" or inflammation. In this case the overuse is acute and generally within a week of it starting to hurt. Depending on the amount of aggravation caused, ¢.g., how. much the pain is ignored and worked through, this stage may last up to three to four weeks. If the aggravation is continued beyond this then the injury progresses to stage two,
The second stage is characterized by chronic degeneration where inflammation goes away and the pain tends to intensify. While this usually occurs most significantly during exercise, pain can be present even while not exercising.
The third stage is tendinopathy in which the tendon itself is weakened to the extent that it may rupture. Pain tends to be extremely bad and may be present all the time in the form at some level.
First stage: The two things to look for that place the injury in this stage is that the injury only hurts during exercise and it noticeably improves with rest.
Second stage: This stage is marked by changes in the signs and symptoms of the exercise. Generally, the affected tendon and surrounding musculature will be tight and stiff especially after periods of activity like waking up in the morning. Pain during exercise is variable, but it may hurt even while not excrcising. Sometimes the pain will start to go away after the muscle and tendons get warmed up for exercise which makes you think you can do more. However, excessive exercise should be avoided.
Third stage: At this stage, the pain has developed to be really bad and you should be discussing it with your doctor or physical therapist.
Typical Site:
The typical sites where tendonitis develops with bodyweight exercise are:
Medial epicondylitis (inner elbow — Golfer’s elbow) which arises from excessive high intensity pulling exercises.
Triceps tendonitis (elbow) which arises from excessive high intensity pushing exercises.
Biceps tendonitis (elbow) which arise from excessive high intensity pulling exercises or shoulder compensations.
Wist tendonitis (wrist) which arises from overuse at the computer or in excess flexion/extension of the wrist. Knowing how to distinguish this between some other wrist injuries is discussed later.
Stay away from painful exercises
Pain is your body telling you that something is wrong. Listen to your body. Continual aggravation of the injury will make it worse and significantly hinder your training.
One to two weeks of total rest should clear up mild forms of tendonitis because the initial inflammation will promote healing. Realize that this does not mean you have to cease workouts altogether but just the exercises of the injured body part. Non-painful mobility work should be executed during this time.
If the rest is successful, work your way back into exercise by starting with 40% volume and adding 10% more each week as it’s very easy to aggravate again. If you feel any twinges of pain or aggravation, immediately back off for the day. It is better to be conservative than to have a chronic condition.
Unfortunately, chronic tendonosis may not respond favorably to pure rest. If your tendonitis does not clear up after two weeks of total rest then you probably have a chronic condition. This needs to be treated different than just mild tendonitis: rehabilitation exercises are needed to stimulate the inflammatory process (along with massage) to promote healing. Any other exercises that use this affected area should be eliminated.
The purpose behind massage is to promote blood flow to the area for healing as all tissues need to have nutrients delivered and waste products cleared from the area. Massage also helps improve tissue quality through helping to release and reorganize the tissue via the body’s natural inflammatory processes
plus break up any scar tissues or adhesions that may be limiting proper movement of the affected and surrounding area
Cross friction massage and myofascial release should be concentrated first and foremost toward the tendon and secondly to the immediate local area within one inch of affected location. Start out very lightly as the tendon may be sensitive. Soft tissue work that is too aggressive may further aggravate the injury.
To ensure the surrounding musculature is operating correctly and not causing excess strain to the affected area, continue to apply cross friction and myofascial release to the whole area in between both joints that surround it. For example, with medial epicondylitis, massage all of the muscles between the shoulder and wrist; with patellar tendonitis, massage all of the muscles between the ankle and hip. If it is an option, using alterative manual massage techniques may help. Graston technique, ART / trigger points, foam rolling, and golf or tennis ball rolling are all great methods to work with.
Note: If one has been through physical therapy and the therapist did not use significant amounts of manual massage therapy then his or her ability as a therapist is questionable in my opinion. Besides rest and ice, which most doctors and physical therapists recommend, the number one thing that will help the most is massage and/or self-massage.
Like massage, icing helps limit some pain and excessive inflammation (which is characterized by edema) especially when done immediately after exercise or prehabilitation work. Additionally, after being iced the body tries to warm up the area and thus promotes blood flow to the area.
Two approaches to icing are generally accepted. Either ice for sessions of 10 to 15 minutes and complete two to five sessions per day or simply ice every other hour on the hour. Direct ice massage on the skin tends to work the best, but avoid getting frostbite.
Alternatively, heat can be beneficial in certain situations. It usually helps most for non-acute overuse injuries afler a week or two of acknowledging the condition and starting to work towards fixing it: at that point the body has had some time to heal
If ice does not help your condition then do not use it. There is no reason to use ice if it does not help.
Chronic cases tend to respond a bit better with heal. If ice is doing nothing and you suspect a chronic case of tendonitis (it has been around longer than multiple months) then heat is a viable option.
Stretching is aimed at the agonist muscles (c.g. the muscles that connect to the tendon in question) because they are usually tight and short from overuse which may contribute to excessive strain on the tendon. On top of that, when there is distinct overuse on one side then there is usually an existing muscle imbalance. Both of these tend to put more stress on the joints and supporting structures such as the tendons and ligaments. Therefore, correcting the imbalance and loosening tight muscles should help get the tissue to function properly.
As a small side benefit, the eccentric nature of stretching creates a gently stimulate the body’s natural inflammatory process for healing.
ceptable microtears which will
Focus the stretching on the agonist muscles connected to the tendon and focus the strengthening for the antagonistic muscles on the opposite side. For example, with medial epicondylitis at the elbow, stretch the forearm flexors and do strengthening work for the forearm extensors. For patellar tendonitis, stretch the quads and strengthen the hamstrings,
This protocol is mostly for chronic tendinosis cases that are not alleviated with solely rest. Eccentric exercises help because they induce small amounts of microtearing which is part of the inflammatory process to promote healing. Bear in mind that sometimes the musculature at that joint will become unable to properly execute a movement because of compensation for the pain. If this is the case, the training of eccentric exercises also helps reeducate the nervous system to fire correctly again
Start with a very light weight and work on the eccentric portion of the lift slowly and assuredly. The eccentric movement should take five to seven seconds.
After it starts improving significantly you can add in the concentric portion. Be careful not to overdo it as it is very easy to aggravate. For something like medial epicondylitis you should choose something to strengthen everything in the forearm such as rice bucket exercises
uch as
It tends to be best to start with very light weights at 40% of 1 RM and open chain exerc eccentric flexion wrist curls (medial epicondylitis) or eccentric leg extensions (patellar tendonitis). You can use the other am/leg to help the other arm/leg up for the concentric phase. This approach makes it easy to load the joint with light weights (dumbbells, ankle weights, etc.) and make very small increases in weight to continue a safe progression.
As you progress, you can move on to more closed chain exercises such as the eccentric of walking down stairs slowly or negative pullups. Close chain exercises tend to use a larger portion of bodyweight, S0 progressing to them too soon may be detrimental to the healing process if they are too difficult and aggravate the injury.
Eccentric exercises that are any more than slightly painful will probably be detrimental. As a golden rule, there should not be any pain at all, but if all exercises are painful then make a reasonable, safe attempt to do the least painful and stop if the pain gets worse.
Cortisone shots may be a helpful option as it has shown improvement in conditions such as lateral epicondylitis. Repeated use of corticosteroids may lead to detrimental effects, so make sure that cortisone shots are being accompanied by proper rehabilitation work to get the best out of your healing
Next, many of these other modalities are highly dependent on the person to whether they will help or not. If you the above options and physical therapy have been exhausted then it may be a good idea to try some of the modalities below in conjunction with the above protocols if you want to avoid surgery.
Rescarch on joint, tendon, and cartilage health supplements varies. Anecdotally, it seems to vary from person to person.
First and foremost, I recommend pursuing physical therapy first as that is a better use of money. But if you want to try various other methods such as
supplements then feel free. Typical supplement purported to help tendonitis, cartilage, and joint issues are:
Glucosamine and chondrotin sulfate (together at a 3:2 ratio respectively), Methylsulfonylmethane (MSM), cissus, S-adenosylmethionine (SAMe). Universal’s Animal Flex has gotten a lot of praise from bodybuilding forums (so take that for what it is worth). Fish oil does a whole host of good things and will be talked about a bit later.
The results from dry needling, ultrasound, and electrical stimulation are variable.
Other modalities that have some scientific evidence backing them are low level laser therapy, platelet tich plasma (PRP), autologous blood injection, and prolotherapy.
I have seen some good testimonials with the LLLT, PRP, prolotherapy because help with natural inflammatory healing process. Therefore, I would recommend checking out those options first especially before any potential surgery.
Surgery is the last ditch option because of the potential for infections and the often sub-par ability of humans to do what the body should naturally do itself.
This is my new stance on this subject.
NSAIDs while great for pain relief often help slow the healing rates of issues that you are trying to fix with rehabilitate. For example, typical NSAIDs prescribed for pain and inflammation are over the counter drugs such as aspirin and ibuprofen. Things you may typically get with a prescription are stronger such as naproxen.
The mechanism of typical NSAIDs is to inhibit the cyclooxygenase pathway of inflammation. This is great because it eliminates the pain by inhibiting the PGE substrates that aggravate the delta and C sensory fibers within the area. However, this is bad because it also the prostacylins and HHTS which are responsible for drawing in white blood cells and platelets that help clean up the damaged tissues, and release growth factors to move on to the proliferation phase of healing.
In regards to Tylenol/Acetaminophen, it is not the same as the other NSAIDs, but it is in fact actually not and anti-inflammatory agent. It reduces pain specifically through the CNS and not at the inflammatory process level. Thus, if you are having trouble with pain, it would be recommended to take this over any of the NSAIDs because of healing rates.
This also applies in reverse though. If you suffer a traumatic injury to the ankle such as a sprain and it is inflamed and swelling up, then we would want to avoid acetaminophen in this case. It is not going to help with what we nced which is the anti-inflammatory factors. We would want to do the RICE protocol, NSAIDs, massage, mobility work, etc. in these cases.
I would try to avoid using NSAIDs for anything related to pain where tissues need to heal. The cyclooxygenase pathway is a critical step of that inflammatory phase that is needed for any sort of tissue regeneration whether it be muscle, tendons, ligaments, bones, etc. If it hurts bad then use different anti- pain medications like Tylenol. It’s only when the inflammation gets so out of control such as with lots of swelling or fever where NSAIDs start to become more useful.
Warmness of the skin area is a good indicator of acceptable levels of inflammation (as prostagladins of the eyclooxygenase are fever inducing). When there starts to be a lot of redness and swelling symptoms it may be time to help cut down on excessive inflammation with NSAIDs. For example, a couple days after workout the muscles are usually warmer because of the inflammation and healing process that is is unlikely unless there is severe DOMS or thabdomyolysis that any NSAIDs may be needed for
It can be argued that any time there is pain then there will be excessive inflammation. Therefore, NSAIDs would actually help healing rates. My stance on this is that if they are helping then continue with it. If they are not helping then do not continue with it. Aliernatively, if you are healing without them then do not bother with them. There is no reason to throw comp
Fish oil is also a good anti-inflammatory if needed, and of course eating right is going to help the most.
These are things are probably not told to you by your doctor or any other healtheare professional (heck, I didn’t even know about NSAIDs vs Tylenol until I was taught that in class a few weeks ago). Keep this type of stuff in mind.
Integration with regular workouts is the same. Perform you workouts in the structure suggested in chapter 14. Remember, the concepts of intralimb, opposite limb, and other body part exercise. If the workouts require use of the injured limb and does not aggravate it, then make sure the tissue is sufficiently warmed up before doing anything.
Proper structuring of the modalities listed above is important. Here is a general guideline of how you can structure a rehabilitative session.
So for example with something like medial epicondylitis I would perform for the tendon specifically:
Additionally, for muscle strengthening/stretching we would want to perform:
So for example with something like medial epicondylitis I would do:
Obviously, you would not split these two things up into specific sessions. You would combine the sessions to work on all of the warm up, eccentrics, massage, stretching, and modalities each in order to minimize rehabilitation time.
Remember, having an injury or something you need to add in prehabilitative work does not mean that you should rest everything and neglect other training. If you have medial epicondylitis (elbow tendonitis) for example you can still do legs and core work as well as to other skill work for your sport and corrective nature things such as flexibility/mobility.
One of the big things with tendonitis at "stability" joints such as the elbows is that there tends to be a oss of mobility or strength in the wrists and shoulders. This may add more stress on the elbows. The same thing occurs with tendonitis at the knees and losses of mobility or strength at the ankles and hips. Thus, if you have tendonitis at the elbows or knees you should work on improving the flexibility and mobility of the two joints surrounding it
Here is a general rule to distinguish chronic tendonosis from tendonitis:
All of these types of symptoms may indicate that the condition has progressed from tendonitis to tendonosis. Therefore, be wary about working through pain. Also, try to figure out what exercises were the offending culprits and eliminate them for now.
As we discussed a bit before chronic tendonitis (tendonosis in reality) tends to persist even with rest. With this in mind we need to make alterations to rehabilitative processes.
Since there is no inflammation present in chronic tendonosis we need to create some to initiating the healing process and improve blood flow. Thus, eccentric exercise becomes the most important part of our rehab routine. In addition, ice tends to not help as much for chronic cases; thus, we want to use heat instead.
In tendonosis there is chronic degeneration of the tendon. Thus, we do not want to massage the tendon itself so much (you can but it needs to be lightly). We want to focus more on releasing the tension on the tendon by hitting trigger points or tight areas in the surrounding musculature. ART, myofascial or cross friction techniques work well for this.
Additionally, mobility to get blood flowing and any fairly non-painful movement is good. Thus, a rehab program for a chronic case would look more like this.
Tee can also be substituted in if it helps more than the heat, but like I said heat tends to be better for those chronic cases that are not healing with rest.
As the condition improves, we want to start to work slowly from the isolationist high repetition exercises into lighter compound movements. From there, you can slowly work back into heavy exercise. The general rule for how fast to go with a chronic case is to take a week for each month you have had that problem. So if you have had this problem for longer than a year expect that it may take upwards of 10-12 weeks to completely rehabilitate yourself back into the heavy weights or high volume that you were used to before you were injured.
Muscle strains, pulls, tears, and ruptures are all different names that describe the same injury conditions. The only difference is in the degree of injury sustained. For example, we tend to think of a strain or pull as less serious than a tear or rupture. To keep it simple, 1 am going to refer to them all as strains from now on.
In this article we will discuss how these injuries arise, how to identify them, and how to rehabilitate them.
A strain occurs when the amount of force put on a muscle is greater than the ability of the muscle to generate an opposing force. This most often occurs during high speed movement; however, it can aceur during sustained contractions. It most often occurs near the end of workouts when muscles are fatigued and cannot generate as much force is in the beginning of a workout.
This means that strains have a higher frequency of occurring:
Now you may have heard that muscle damage, especially factors related to the damage such as delayed onset muscle soreness, is caused by eccentric muscle contraction. This is true. The same thing occurs with strains. They always occur during the eccentric contraction of the muscle.
Even in cases where a strain occurs during a *concentric’ contraction are actually during an eccentric right at the time when the concentric motion is switching to the eccentric contraction.
For instance, if you are one who tends to arch/crane your neck by looking up instead of keeping head neutral during deadlifts, squats, and pullups, the impingement of the nerves that come out from the cervical plexus may inhibit force output during the movement. Thus, as the movements move into the eccentric phase, the body may not have enough museular force to exert to slow the movement down and the muscles may strain. This is one of the major reasons for correctly executed these techniques as well as the fact that craning the neck often gives people pain and tight muscles as well as headaches.
Hamstring strains occur when the knee is moving forwards or the foot is receiving the ground as the hamstring is lengthening. Back strains occur during deadlifts as the back is rounding and the spinal erectors are lengthening. Biceps strains occur as you are coming down from the top of a pullup.
Therefore, knowing the factors that increase propensity for strains is important. Thus, if you are getting older, having poor technique, poor flexibility and mobility, tight muscles, or are weak and do intense workouts you may be more susceptible to strains and need to be more careful with operating at higher intensities.
Obviously, if you have previous medical issues or strains you will know that you need to be proactive. If you are doing intense workouts at high speeds, save the static stretching for afterward unless you have flexibility detriments that need to be addressed prior to workouts to ensure safety during the workout.
As we discussed strains always occur during eccentric loading of the muscles.
This means that during sprinting in the hamstrings they will tend to occur during the phase where the foot is starting to receive the ground as that is where the muscle is at its longest. Groin strains (at least adductor magnus) tend to be similar. The other half of groin strains — the hip flexor strains, adductors longus and brevis and pectineus — occur on the opposite side of the stride where the foot is starting to leave the ground to come forward.
In kicking sports strains will tend to occur after kicking the ball extremely hard as the leg travels up and forward in front of you.
Strains during lifting such as the back tend to occur when technique breaks down because of fatigue and the muscles lose their isometric contraction such as during squats and deadlifts when the back starts rounding. Likewise, in the upper body they will occur on the descent of pullups for the biceps, the descent of the dips for the triceps, and lowering the weight halfheartedly or jerky.
This is why it is important to keep strict form especially when you are getting fatigued because that is when they are most likely to occur.
When a strain occurs you can recognize them through the fact that they:
Strains are graded on a 1-3 scale.
Grade 1 tears consist of minor tearing of the muscle. There is no bruising and little to no swelling, but the pain is present in the soft tissue. The amount of pain is often variable to how the person perceives it. It is possible that there is no pain on concentric movements and only eccentrics. There is unlikely to be major pain with some light pressure to the area, but there may be some discomfort or minor pain. This is what most often occurs with people who workout.
Grade 2 tears are partial tears of the muscle. There is likely to be some swelling. Bruising is still variable but most likely will occur as the tissues are damaged/ruptured enough that there will be blood leaking out. Both concentric and eccentric movements will hurt, and putting pressure on the area will cause pain. Since the muscle has a large injury it will resultin limited range of motion. Often the muscles will start to get tight to help protect the rest of the injured tissues.
Grade 3 tears are complete ruptures of muscle or close to it. There will be swelling and bruising. There is also likely to be a divot/gap left by the muscle where it tore in two. It is important that if this occurs to throw RICE it right away — rest, ice, compression, and elevation — and to get to the emergency room ASAP to get it checked out
I would also advise going to the ER in the case of a grade 2 partial tear as well, but it may not be necessary depending on the circumstances. In any case, this article is mostly directed at grade 1 and low grade 2 strain prehabilitation and rehabilitation.
If you are weak you need to get stronger. If you have very tight muscles it is imperative to increase mobility in those muscles through static stretching and/or proprioceptive neuromuscular facilitative stretching after your workouts. If you're getting up in age, you definitely need proper warmups before workouts. Save your static stretching for after workouts except for where you need it to maintain proper technique.
And, most importantly, always maintain proper technique. If you are doing timed workouts it is important to always emphasize technique over getting a faster time. Constantly drilling technique is the key to success in every sport and athletic endeavor. You are not doing yourself any favors by short cutting yourself to look or feel better, and you increase your injury risk. It is a lose-lose situation.
The acute phase in all injuries is characterized by tissue damage that elicits an inflammatory response in the muscle. Swelling and bruising may or may not be present. If they are it is all the more necessary to take the proper steps to encourage healing of the tissues.
In general, PRICEM - protection, rest, ice, compression, elevation, and mobility — is prescribed. The the ICE part will be critical to reduction of swelling and inflammation within the first 048 hours. Afterward, compression will be the biggest factor in reduction of inflammation so it would be wise to ry. Obviously, you will want to protect it from more damage, so if it hurts to walk try to stay off of . inves ive material to limit swelling if necess
n some compres
Also, within this first period reduction in inflammation is critical to speed the body’s recovery processes. Inflammation is a natural process which helps stimulate healing through increase of blood flow to the area but blocking the blood flow out of the area as well as increasing the amount of immune response to the area. This is great when we are sick to promote recovery; however, in injuries to our bodies the inflammation is overkill and actually prolongs it. Thus, we want to reduce it a fair amount.
If the pain does not significantly reduce within about a week, I would schedule an appointment with a doctor to have it looked at. This may indicate a more serious type of strain.
This is the M part of the PRICEM.
First, strains should never be stretched because that is typically how they were injured in the first place. However, it is important to keep the body part moving as much as possible without causing pain. This is because of the inflammation and the scar tg that is about to be formed. In add: traumatic injury the muscles tend to tighten up and lock down to prevent further damage. These factor will impede the healing processes.
n, in any
If there is excessive swelling use your hands to push the swelling up towards the heart, This will help clear it out and speed up healing.
Massage in this phase should focus on light/superficial massage to the surface of the skin moving swelling and inflammation out towards the heart. Do not push into the tissue hard or do anything that causes significant pain as you will be interrupting the healing process. But light soft tissue work is good to stimulate the blood flow and help organize regrowth.
Most doctors for grade 1 or 11 strains will slap you with a prescription of NSAIDs and possibly a couple other drugs (to counteract the affects of strong NSAIDs) and tell you to RICE or rest.
This is not bad because it works, but my preference is with the strong anti-inflammatory effects of fish oil. Fish oil not only had great side effects such as better overall health through improvement of cardiovaseular risk factors and improvement of depression, schizophrenia, etc. Since most of us have problems with inflammation in the modem age (from eating too many refined carbohydrates, and grain fed meat), reduction in inflammation is extremely positive on healing rates.
Also, eliminate processed food out of your diet and make sure you get a lot of sleep because our bodies heal the fastest during rest.
The water soluble vitamins such as the B-complex vitamins help promote healing as they are needed for tissue regeneration and repair. However, if you are already eating a well balanced diet of meats, fruits, and vegetables you are already getting enough of these vitamins.
In acute phase damage inflammatory processes tend to cause a lot of oxidative damage. Thus, taking increasing dosage of vitamin C which is an anti-oxidant is good. Increasing A and E which are also anti- oxidants are good 100, but not too much because they are fat soluble. The same is true of other supplements such as Coenzyme CoQ10 (ubiquinol) or acetyl-L carnitine.
Fish oil i vastly more important than these though so if you are going to spend money on anything let it be the fish oil.
Usually these phases are separated. However, repair and remodeling do occur simultaneously if the muscle is taken carc of properly. Thus, I am grouping everything together.
The body in this stage is basically repairing what damage it can, breaking down what it cannot repair forming scar tissue and laying down new tissues.
This phase begins within about 48-96 hours after injury; however, we are going to take a bit morc conservative measures. Basically, once the tissue starts to feel better with your movement that you are doing everyday from the acute phase, and the swelling is reduced we can consider ourselves in this phase.
This is important again to help keep excessive inflammatory processes down. Vitamin C and B complexes in large amounts as well as enough of vitamins A, E, and other anti-oxidants are great.
Since the swelling is reduced and the anti-inflammatory fish oil should keep it in check, we can move towards heating up the muscles.
The benefits of heating is that it helps increase blood flow to the muscles. Heat will also loosen up the tightened muscles to allow improved movement capabilities. Keep up the paines movement.
The massage is to be maintained, but the main focus of it now is to loosen up the tight muscles. Add in very light stretching work after to help increase the range of motion. This is in addition to the already frequent painless movement
The massage plus stretching here can be deeper, but still not harder to cause pain. You can start to hit those deeper tissues and stimulate blood flow to them as well as help reorganize the tissues more correctly.
Programming in this phase may follow these steps:
Like in tendonitis we first want to start with very light weights 1o give us a good degree of control over the movement to make sure we do not restrain the muscle. Remember, we are only a couple days or weeks out from major damage to the muscles, so it will be very easy to reaggravate it.
If it is possible to do some isolation work with the muscle without causing significant pai aggravation then this is a good option. Keep the weight very low and only do a few sets of 15-25 reps. Now is not the time to be aggressive with the weight increases. If there is any type of twinge back off immediately. We want to work higher repetitions to build endurance because the tissue will be extremely vulnerable when fatigued.
or
Likewise, with an injury that cannot be isolation such as a lower back strain, isometrics can be supplemented instead. For example, non-weighted squats or back extensions or very light deadlifts/good mornings can work. For back strains specifically I like reverse hyperextensions. Be very careful though.
At this phase we are looking to exercise, and then allow the body total healing over the next 24-48 hours. So only reintegrate exercise to 2-3x a week, and keep the progressions small. Being extra cautious will save you more time than having to come back from a restrain which can often be worse than the first one since the tissues are already more vulnerable to take more damage.
Slowly progress your way from isometric exercises by increasing the intensity. Once you have strengthened the area sufficiently, work your way back into light compound exercises. From there, progress the intensity in your compound exercises. From there, it is just a slow progression working your way back to full workouts.
Like we discussed earlier strains are more likely to reappear in those with previous strains. Thus, it is important to do a few things to prevent another strain.
Improving mobility and flexibility is a major factor. This work should be integrated into your warmup and your cool down. Add in some soft tissue work such as foam rolling, and self massage. Do dynamic and static stretches when appropriate. Add in mobility work.
The second is to make the muscle more resistant to damage. As you know, eccentric movement is when the majority of damage occurs during exercise. However, the muscles themselves gain a resistance to the damage with repetitive eccentric work. The model by which this occurs is the "popping sarcomere theory" which we covered in a previous chapter.
To sum it up, during eccentric exercise individual sarcomeres distend during the lengthening of the muscle which accrues as damage (excess sarcomeric distension in a localized area is a strain). The body responds to this micro damage by adding additional sarcomeres to the muscle during inflammatory phase healing process. Subsequently, the muscle becomes more resistant to damage because of its ability to take damage.
This means that the major aspect of prehabilitative work should focus on slow eccentric exercise which we already deseribed in the previous section. This is especially true with explosive movements, Thus, for a sprinter with a hamstring or groin strain we want to focus on eccentric hamstring curls for a 6-
10s negative phase for higher repetitions. Then we will decrease the repetitions as we progress.
From then on progress in our prehabilitative work to a 6-10 second count eccentric on the eccentric portion of compound lifts such as deadlifts, good mornings, hyperextensions, Romanian deadlifts, etc. As we stated earlier, do not be too aggressive with the weight and be careful to maintain strict technique.
All in all strains are not that complicated to deal with if they are grade I or low grade II. Higher grade 11 should be treated exactly like these except the acute, repair and remodeling phases will take much longer. Grade III tears you should discuss with a qualified medical professional
The hard part is making yourself take care of your body through the protocols mentioned above. Be disciplined. Do not take your body for granted. Think of it as a learning experience that you care not repeat. Do proper mobility, prehabilitative, rehabilitative work, and focus on your technique.
All of the things I have stated in this article area critical for speeding the healing processes. However, there are natural limits to your healing ‘you strained yourself bad enough. Of course, healing can be improved by sleeping more, eating quality foods, etc. as well as the RICE, massage, fish oil, etc. Be sure to take care of your body, and it will respond in kind.
s going to take some tim
Tension headaches or pain near the base of the skull during exercise tend to occur for a couple of reasons,
If the headache occurs during exercise and/or only occurs during or shortly after exercise then it is likely that there may be some improper form or tensing the muscles too much during the movements
For example, many people get headaches during squats, deadlifts, and pullups. This is because they are really straining to keep the back straight an are by extension arching the neck strongly, or craning the neck trying to get the chin to the bar. For bodyweight movements these may occur during pullups, dips, handstand pushups, or anywhere that the head is excessively hyperextended during any type of movement. This shortens the muscles at the base of the skull and may cause them to cramp giving you tension headaches. Also, the tight muscles may cut off blood flow to the brain which may also give you a headache.
These types of excessive movement are also important to eliminate because they decrease force output. When you arch your neck or crane it you are decreasing the space between the vertebrac that the nerves to your muscles come out of to go to your limbs. When you compress nerves the body will think it is being injured and will decrease force outputs to the muscles to avoid them from being impinged too strongly. Thus, your force output will decrease. Proper form is not just to help from being injured — it also allows us to express our power and strength optimally to get a better training stimulus,
Besides focusing on fixing the technique, there are multiple modalities that can be used to help get the body back to normal. Heat and neck massage to loosen up the muscles in the neck area tends to work very well. Similarly, mobility work by taking the neck through non-painful range of motion before exercise and after exercise is effective. If you find particularly tight muscles or areas then more static type of stretching may be recommended. A combination of those four modalities will fix most of these types of problems if this is the actual issue.
Remember, the main thing is that you should make sure that during the exercise you are keeping the head neutral and not straining the neck muscles too much.
If you are worried that it could be symptomatic of something more insidious you should get it checked out by a doctor.
This injury tends to manifest as pain along the sternum or the chest area where the ribs/costal cartilages connect into the middle of the chest. If there is pain decper in the chest have it checked out by a doctor.
This injury tends to occur in people who have not used rings before or are starting bodyweight training at a basic level of ability. It will happen when there is intense use of the pectoral muscles. For example, exercises such as rings tum out support work, rings pushups, rings dips, or any other type of pressing that uses the chest a lot may begin to hurt along the sternal area. Back lever and front lever have been known to aggravate this condition occasionally.
Since the origin of the pectorals is on the sternum and partially on the costal cartilages, if you have not used your chest in resistance training much before the connective tissues are not as strong. Thus, when you do a deep movement where you really stretch out the pectorals like dips, the origin of the muscle on the costal cartilages can start to pull them away from the costal facets on the sternum.
Obviously, this creates inflammation and in general can lead to some popping and hurting. The main thing to do for this injury is to rest and let it heal,
Ice if it helps. Otherwise, once it starts feeling better use heat to stimulate more blood flow to encourage faster healing from the body since the area does not get a lot of blood flow as it is bone/cartilage in that area.
Keep the muscles working through full but non-weight bearing and non-painful range of motion so that the muscles do not tighten up on you. The muscle movement will also help stimulate blood flow to the area as well.
Anti-inflammatories/NSAIDs can be used to help deerease inflammation and allow healing to occur may help if it is particularly bad. Fish oil is always good. Massage to the area to increase blood flow will help as well.
Usually if you do not keep aggravating it, you should be able to get back to exercising within a week or two.
Just avoid the exercise that aggravates it for a while, and focus on other exercises that are less intense of the chest. Then work your way back inta these slowly so you do not reaggravate the condition. Be very careful as it is easy to aggravate repeatedly.
Pain in this area can be for a variety of reasons. Generally, as I stated in previous chapters I would recommend getting any type of pain with the scapulas/shoulder area checked out by a physical therapist or qualified professional. If you have chronic issues with the thoracic spine, scapula and ribs, because the issues are not always where the pain is located. However, let us discuss some general concepts and take a Took at what particular things can be tried if you decide against professional help.
If the pain is in the neck or thoracic spine area within about an inch and you have trouble moving in one or more directions then this tends to be indicative of a vertebral facet or rib issue where it lips out or subluxes slightly. Sleeping awkwardly or moving quickly can make this occur. I would not be worried about these unless it persists for more than a day or two without improving. Usually, they will spontancously resolve as long as you stretch out tight muscles and keep moving. However, if it does not resolve in a couple days or it gets worse then I would highly suggest getting to a chiropractor or physical therapist ASAP to pop it back in place. If you do not and it stays there and the tissues start to get used to it then getting it to stay in place after manipulation may require multiple visits to a professional rather than just one or two. Not exactly what you are looking for when trainine.
Issues that are in the muscle bellies around the scapula(s) can be there for a variety of reasons. There are some great mobilization techniques you can do with a lacrosse ball or tennis ball by rolling around on the tight or sore areas to help loosen them up. Foam rolling and other stretching exercises to all of the muscles in the arm and around the scapulas including the chest, anterior and posterior shoulders, back and lats are probably good to try as well. If this resolves the issue then that is great. If it does not resolve the issue or it is chronic then there is likely something else that is wrong. I would suggest getting it checked out by a professional if that is the case.
If the issue is bilateral then that tends to indicate more of a postural or structural issue. If the issue is unilateral then it depends on a few factors including technique, possibly overuse, dominant vs. non- dominant sides, scoliosis, etc. These are not hard and fast rules so self diagnosis is not really recommended.
Again, if pain is sticking around and not receding after a week then it is a good idea to get it checked out by a professional. Why let nagging issues bother you for a long amount of time and hinder your training?
Generally speaking, low back issues will probably not happen to you while performing bodyweight exercises. However, it is possible that they can result from rounding the back too much during stretching. Likewise, if you are training the lower body like I suggest with squats, deadlifts, and other good compound exercises, you may run into some trouble with the low back at one point or another. Therefore, I will include cover this topic.
Lower back pain and injuries are common among weightlifters and even non-weightlifters. Shoes and sitting as well as very poor posture and biomechanics may exert have chronic detrimental cffects on our bodies. Combine this with poor technique, especially in lifting objects off the ground or during working out, and you have a recipe for injury, pain, and inflammation.
This short section is not going to be an end all article on how 1o solve lower back pain and injury. Rather, there arc categories of lower back injuries that all need different attention depending on what has been injured. From there we can determine what the best course of action that needs to be taken for each individual because everyone is a bit different.
Flexion based injuries from lower back rounding tend to fall in 3 different categories.
These are the three generalized categories. We will learn how to identify which one you may have, and then how to obtain professional treatment if required or rehabilitate it yourself.
Other types of injuries are not very common and if obtained from lifting in particular may represent some inherent structural deficiency or faulty connective tissue usually due to genetics or improper nutrition.
If you suspect you have an injury that does not fall into any of the three categorics above see a medical professional immediately. Also, if you have an injury which presents debilitating pain or presents possible insidious neurological symptoms such as sensory or motor deficits see a medical professional immediately. Motor deficits are critical enough that you may want to g0 to the ER ASAP.
Bulging and hemiated discs will manifest pain on, in, or around the spine itself. If you can sense the pain in the direct center of the back, it will be one of these problems
If the bulging or herniation is low enough on the spine it may also impinging on some of the nerve roots coming out to the sides. This tends to manifest itself as radiating pain out of the side or lower extremities. These are called radiculopathies (from the "nerve roots" and and the "radiating pain" caused by the impingement/pinching of these nerve roots). We will discuss arm radiculopathies later in this chapter.
The most common case with radiating pain is sciatica. In this case, a bulging or hemiated disc in the low lumbar region (aka "around or just above the butt crack") will impinge on the nerve roots for the sensory and motor nerves of the legs. Sciatica in particular is usually manifested as radiating pain into the buttock region and may continue down farther into the leg even as far as the foot.
For cases like this is it best to go to an orthopedic doctor to be assessed as to the extent of the damage. This may require an MRI as that will show what is going on in there. From there proper treatment can be determined.
often you will be referred to physical therapy for conservative care before any surgery or steroid injections. A good physical therapist should be able to help you work your way back toward working out again.
Do not aggravate this condition with significant activity otherwise it may lead to permanent injuries.
In the meantime, in almost all cases there will be inflammation accompanying the pain. Decreasing inflammation and proper mobility work to decrease the amount of inflammation and pain will help case the symptoms.
If you are eating large amounts of carbohydrates it may be a good idea to eat more protein and fat as carbohydrates are pro-inflammatory. Also, supplementing fish oil is a good idea as well.
For exercise, everyone is individually different with lower back pain. Thus, some exercise may worsen the pain or not help; however, some may help and work effectively. Play around with them and find out which ones work best. Here is a list of exercises to get you started:
In particular, reverse hyperextensions exercises as a strengthening tool tend to be extremely good for rebuilding strength and hypertrophy. About 95% of the people who I have seen have used these to reprep themselves for going back to the classic compound exercises like squats and deadlifts have succeeded.
If any of the above exercises hurt, drop it immediately. Do not come back to it for at least 2-3 days. After that try again as it may help more at the different stage of recovery than initially. The same is true with helpful exercises if they suddenly become bad then drop them for a couple days and come back to them later to see if they help.
The primary thing you will have to focus on the road to recovery is regaining mobility and strength in the ankles and hips, and improving core strength and stability in the arches, knees and especially lower back i this case.
During improper lifting or bending, one side of the muscles may fail a bit earlier than the other. This is common as we all have a dominant side. In this instance if the muscles do not strain or the weight is not immediately deloaded, the SI joint may slip or become rotated causing pain. This also may occur if you take a significant impact more on one leg than the other such as a uneven landing in gymnastics, parkour, martial arts, etc. Likewise, if significant eternal forces are generated through one leg or on one leg this can occur as well.
SI joint problems tend to manifest pain right above the butt crack and an inch or two to the right or left depending on which one has slipped or rotated. It is a very similar pain to the lower L4-L5 and L5-S1 disc issues like discussed above, and a slipped SI joint can manifest in sciatica and radiculopathies as well.
If you run your hands down your sides starting at the ribs, the first bony protrusion you will encounter is the iliac crest. This is at the level of the L4-LS disc. If you follow the iliac crest backward with your hands as it slopes downward you will encounter your SI joint where the pelvis meets the sacral vertebrac. The SI joint is about 3-4 inches long so the pain may be anywhere along it. If the pain is located there you may have an SI joint issue.
A slipped SI joint will also manifest in one leg being functionally shorter than the other. If when you locate your iliac crest if one side is higher than the other this will indicate an SI joint slip. However, a rotated ST joint may not manifest in a leg length discrepancy, so this is not always an indicator of a problem
Thus, if your pain is (1) 1-2 inches off center from the spine, (2) is an 1-2 inches lower than the iliac crest level, and (3) feels in the bony region of the pelvis it may be likely have you have an SI joint issue. Same with the functional leg length."
See a chiropractor or physical therapist. Competent health professionals in these two areas should be able to fix your dysfunction by popping you back into place or resetting the pelvis.
It is important that you limit pain and inflammation again with fish oil and rest. Do not aggravate this condition.
Since the SI joint may be rotated and slipped, some muscles will be shorter or longer than usual. When this occurs with injuries, the tendency of the body is to lock down the muscles to prevent further injury. This is not good especially if you can get to a chiropractor or PT quickly. So what we want to do is keep the muscles loose with massage and possibly some heat. However, heat should not be placed on the SIjoint - just the lower back and possibly the hip muscles as well).
You may be able to check yourself with the long sit test. When supine or on your back, your legs will be uneven lying (c.g. pelvis oriented upwards). When you sit up with the legs straight (long sit) they will be even because the slip does not manifest when the pelvis is oriented forwards. If you find this is the case, definitely see a professional immediately. Also, even if this does not work but you still suspect something I would see a professional anyway.
It is possible to reset the pelvis by yourself and/or another person, but if you are not confident do not try these yourself and get yourself to a quality health professional
One of the manipulations you can do is with a doorway . Another is squeezing a semi-hard object between the knees. I am not going to provide pictures or describe how to do these in this book, but there are some manipulations you can try yourself located on youtube.
Strained and pulled muscles will be located to either side of the spine in the muscle belly of the tissues. Strains will usually occur during lifting and in the spinal erectors — iliocostalis, longissimus, and spinalis — although they can occur in muscles such as the quadratus lumborum or others.
If your lower back pain is below the ribs and above the SI joint in the muscles, then it is likely you have a muscle strain.
In the case of muscles strains or pulls unless it is extremely bad where your tissues are tuming black and blue and you absolutely need pain killers, you probably do not need to a see a doctor. This is because you will most likely just get a prescription for pain killers and be told to rest.
However, if you are that worried about your injury then do not hesitate to see a doctor. Better safe than sorry.
We have already talked about muscle strains, their etiology, and rehabilitation earlier in this book! See that section which is located earlier in this chapter.
Generally speaking, if the "injury" i muscle bellies and not in the SI area, then it is probably a muscle strain.
more than about 2" off of the spine and located within the
Likewise, if the pain is located in, on, or around the spine within about 2 and you have radiating pain then it may be a spinal injury such as a bulging or hemiated disc.
Alternatively, if the injury is much lower in between the level of the iliac crest and the "butt crack" and slightly offset then you may have an SI issue. Like the spinal issues, this may manifest in alternated limb length and/or radiculopathies.
If you are concerned about your injury it would be best to see a medical professional. Depending on the type of injury, the professional you would want to go see may differ. Thus, if you strongly suspect a certain injury, it may be in your best interest to try to get to the professional recommended.
Impingement occurs underneath the acromion. What happens in this abnormal condition is that the Soft issues — muscle, bursas, fascia, etc. — are compressed by the greater tubercle of the humerus against the acromion on the scapula. The pain for this pathology is more superficial (e.g. not located deep inside the glenohumeral joint) and is usually located in the front/side of the shoulder under the outermost bony structure which is the acromion.
This dysfunction typically occurs when shoulder mechanics are thrown off or there is improper lifting. In flexion (arm moving forwards overhead) and abduction (arm moving sideways overhead) the scapula is supposed to rotate upwards and the humerus is supposed to externally rotate to clear the greater tubercle from impacting the acromion.
In certain exercises such as sumo deadlift high pulls or upright rows where the humerus is internally rotated moving upwards it creates ideal conditions for impingement. Likewise, if muscles are tight or bound down that do not allow the scapula to rotate upwards properly then impingement can also occur.
If impingement is suspected rest, non-painful mobility, and ice tend to be the most helpful modalities for this pathology. If it is particularly bad fish oil and anti-inflammatories such as NSATDs may help.
This type of injury is usually caused by predisposing genetics factors in combination with certain risky" exercises and poor technique. The genetic factors are not something you should worry about (e.g. oddly shaped acromion processes). However, the factor that can be control is some of the more risky exercises and poor technique.
Any type of overhead pressing especially with handstand pushups should be take care of to use proper technique. The more flared the elbows are the riskier the movement is to create some type of impingement force on the shoulders.
Likewise, other wide grip or behind the neck exercises such as: wide grip pullups, behind the neck pullups, behind the neck presses, and the iron cross are much more risky for this type of issue to occur. Flared elbows elbows or wide grip tend to place the shoulder in a more vulnerable position because of potential mobility issues and for some like wide grip pullups and crosses the distraction forces on the joint tend to fatigue the rotator cuff muscles much more quickly which allow the humerus to ride up and impinge itself.
Similarly, any type of pulling or pressing exercise that utilize intemal rotation of the humerus in abduction are not good as well. This is not indicative of many exercises in bodyweight except maybe something along the lines of back lever pullups which is why they are not a valid progression that T discuss even though they are seen in certain youtube videos.
The most famous barbell exercise(s) where this occurs which I have already mentioned are with sumo deadlift high pulls and upright rows. I would avoid these exercises in general if you want to avoid shoulder issues.
Acromioclavicular joint issues tend occur more with an impact injuries. These are hopefully not issues that you should incur from bodyweight training. However, for those with loose AC joints or those with previous AC joint injuries that may become aggravated this will be a good section.
The AC joint connects scapular to the rest of the body through the clavicle. The joint is supposed to be relatively immobile, but it does have a small bit of movement which allows the scapula to elevate and twist to allow the arm to move overhead. Once it gets excessive movement via sprain or tearing of the ligaments, it is very easy to get arthritis in the joint since we use the shoulders a lot and there is not a large amount of blood supply to the area the cartilage can degenerate.
What you want to do with AC joint type of issue is rest. Massage the muscles around the area to inerease blood flow for healing and keep the muscles from tightening up. Use fish oil or NSAIDs for anti- inflammatory. Ice if it helps.
Once it start feeling better improve range of motion with non-painful movement, and start strengthening rotator cuff muscles to make the shoulder more stable.
Then work slowly back into compound movements.
Usually each of these steps will take 2-4 weeks each depending on the grade of tearing. It can take more or less depending on how your body recovers. The most important factors for healing in general will be eating correctly and sleeping a lot
If you have a loose AC joint like I do you will notice that your rotator cuff muscles will tend to tighten up because of the relative instability across multiple joints. Make sure you continually stretch them 50 you maintain your range of motion.
One important thing to note is that this must be pain or inflammation at the AC joint. There are a couple of other issue which may seen like the AC joint but are not. For example, pain or swelling either underneath the AC joint or posterior to the AC joint may seem like an AC joint issue but may really be another whole issue altogether. A lot of structures run through the area underneath the AC joint including the brachial plexus and various muscles such as the supraspinatus and other muscles.
This means that if the issue is not directly at the AC joint and under it you may be dealing with something else altogether. If this is the case, it would likely be best to see a professional about it especially if you have sort of radiating pain which will be discussed in the next section.
Radiculopathies dot not describe a particular condition. They do describe a set of conditions where the nerves are typically impinged or inflamed. This may cause weakness, numbness, or difficulty controlling specific muscles.
To be honest with you, this onal about because this is something you usually want to talk to a profe messing around yourself with the nervous system can be a bad idea. I am not even distinguishing between neurits type of peripheral symptoms and true radiculopathies. If you have any questions whatsoever then see a professional.
The interesting thing about these types of issues is that they can occur at any level of the nervous system. The nerve issues can come from the spinal cord, the nerve root as it exits through the vertebrae, the thoracic outlet, all of the splits around the brachial plexus, and anywhere along the named nerves branches that descend into the arm/forearm/hand.
Therefore, an issue that crops up as pain in the hand may have been caused by issues up at the neck, orit could be more why I suggest professionals deal with these issues — al such as at the wrist. This you likely do not know how to figure out at what level they are at or the solutions that are used to correct these issues.
If the prescription of the doctor is to rest and let it heal or you are waiting for physical therapy, there are a couple things that can be done in the meantime that may help. However, remember that you should be dropping offending exercises as they can make it worse.
Nerve glides are great exercises to help mobilize the nerves and stretch them. Like muscles, they can get tight and bound down by scar tissue. Therefore, exercises to mobilize them and improve vascular flow will help improve these issues.
Note that if you have an issue with one of the nerves, it must reproduce your symptoms.
The brachial plexus contains C5-T1 nerve roots that differentiate into five named nerves that supply motor function and sensation down into the arm. Of the five named nerves, two stop up near the shoulder and arm: the axillary and musculocutancous respectively. Three main nerves, radial, ulnar, and median, supply motor and sensation down in the arm. These three will be the main ones focused on because they are longer and thus have the most potential for injury.
Repetitive trauma or workout out where the tissues become tight can create scar tissue and adhesions which can bind down the nerve. When we move, the adhesions or sear tissue do not allow the nerve to move freely and thus create symptoms of pain, numbness, tingling, or coldness in the fingers.
Some studies have shown that nerve gliding and flossing helped to avoid surgery when nerve gliding is added to the therapy program.
It is very important not to over-stretch the nerve during any of these exercises. You want to go to the, point where you may feel the symptoms and then back off. It is best to perform these when you have free time to relax and are in a quict area so you can pay attention to the sensations that you will be experiencing during these exercises. Feeling tension is good but do not stretch to the point that you feel pain or numbness. You may feel tension from the neck all the way to the hand or only parts of this pathway. There is also some evidence that you may feel it in the chest, back or even down into the legs. Nerve gliding on the sciatic nerve can cause some symptoms into the arms as well.
With gliding we are going to focus on:
With flossing we are going to focus on:
There are a couple different methods of teaching nerve gliding exercises. I am going to provide a couple pictures of the ending positions, but if you feel tension and/or symptoms before they are complete then back off and do the gliding or flossing there.
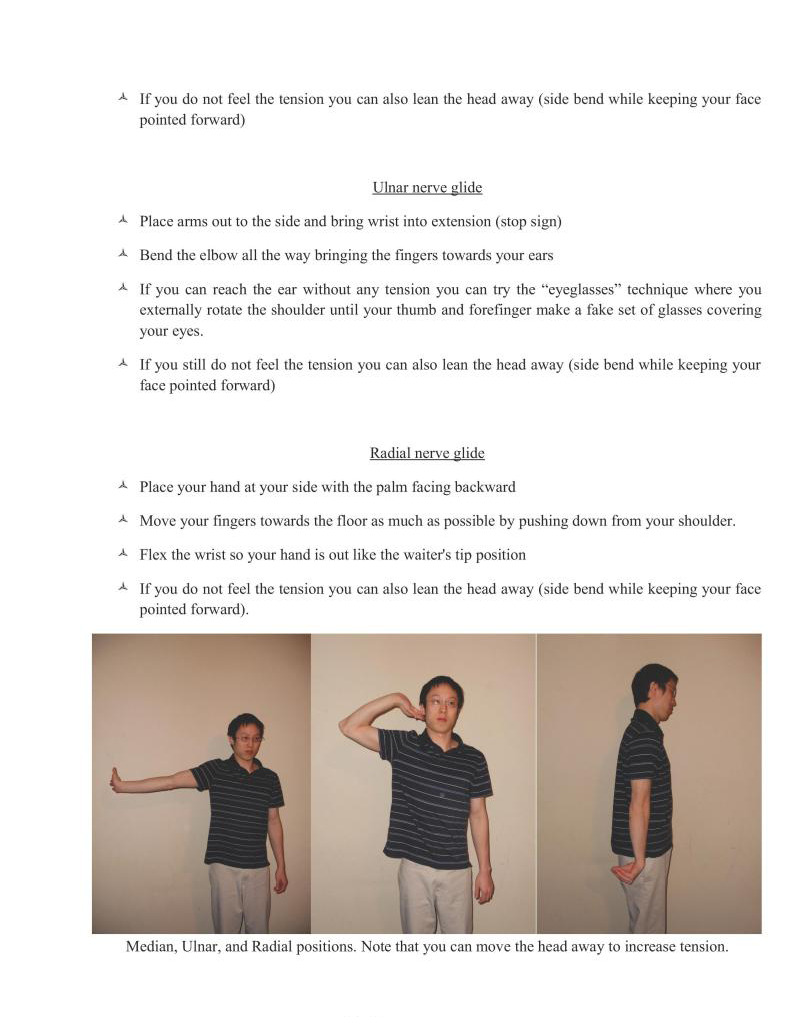
A Place arms out to the side and bring wrist into extension (stop sign)
Median, Ulnar, and Radal positions. Note that you can move the head away to increase tension.
Perform these for a couple of sets of 10-15 repetitions.
Remember that you should only feel tension when you are doing this. If you feel symptoms, you need 10 back off so that you only feel tension. Perform them when you are relaxed in a quict environment and only do them slowly.
Only do these once per day until you can see how your body responds the next day to them. If they are helping, then maybe start adding a second session per day. Build up to 3-5x per day as necessary.
Remember, the goal is to end better than when you started. If you are feeling more pain or numbness and tingling then you have overdone it.
Additionally, any type of stretching, massage, and mobilization work anywhere from the spine down to the point where the radicular issues start is a good idea. Starting to look at posture is a good idea as well,
Carpal tnnel syndrome as its a common problem most people have some knowledge about. Therefore, we are going to examine it as an example.
Carpal tunnel is one of the most common misdiagnosed problems today. There are many things that can cause pain, tingling, numbness, etc. down into the wrist and hand area
For example, tight muscles that can impinge nerves and refer issues down the wrist area are the pectoralis minor, latissimus dorsi, subscapularis, and pronator teres. Other muscles in the neck, arm, and forearm may do so as well not just these four so it may be useful to just target everything and see what helps the mos
Likewise, rounded forward shoulders can cause some issues because of improper tensioning and imbalance of multiple muscle groups around the shoulder which can affect the brachial plexus. One of the biggest spots to hit is improving thoracic spinal posture through foam rolling, lacrosse balls, etc.
Other specific modalities that can be used in combination to help loosen up areas are heat — massage —» stretching to the flexors of the wrist. In that order. Aim to increase mobility in the wrist in that area. 1- 3x a day for 3-5x a week (10-15 mins for heat, 10-15 for massage, 5-10 for stretching).
Muscle imbalances in the wrist can also contribute to the development of this issue so strengthening the wrist extensors may help in combination with loosening up the wrist flexors.
S0 is you can see a lot of issues need to be evaluated in each individual case which is why it is a great idea to see a doctor or physical therapist about this first. But in the meantime while you wait there are some things that can be done that may help start (o resolve or at least make it so the injury does not progress further.
The wrists are vital because they will be supporting your entire bodyweight during many of the exercises. Thus, if do not have a sports background where you put significant amounts of weight on your wrists, then be easier to overuse the wrists or get wrist pai
If you are starting to have wrist pain there is a three step process that you should use to get yourself back on track.
Perform this phase until after it stops hurting to full range of motion. Some of the mobility work I like will be discussed more in Chapter 16.
Rice bucket (opening and closing fingers, rotating the wrists) and seated flexion/extension are two particular exercises that are effective. Wrist pushups are fine as well. Wrist curls are alright as well.
Additionally, extensor specific work is usually recommended because flexors are usually too strong. Do not do compound exercises yet unless they do not hurt.
Use neutral wrist position techniques such as support holds.
Each phase make take a few days to weeks depending on the extent of injury. Discomfort is your guide — do not go into pain threshold. Going to pain threshold and slightly overdoing it may set you back significantly.
The prehabilitation with mobility and flexibility section in the next chapter talks about some of the useful exercises for phases 1 and 2 if need any ideas.
If wrist pain persists and does not gt better after 1-2 weeks I would get it checked out by a medical professional. Traditional overuse taken care of correctly should at the very least start resolve by this period in time. There are many different pathologies where if cartilage is disrupted or the bones of the wrist get subluxed that you cannot fix by yourself. Therefore, persistent wrist pain is best checked out by a professional.
Joint cracking & popping.
The theory on how joints pop and crack is due to cavitation. When the joint is "cracked" the volume within the joint capsule is increased through stretching. When this occurs, the pressure drops within the synovial fluid which causes the small amounts of air dissolved within the fluid to come together and form bubbles. They then collapse on themselves. The formation of these bubbles and collapse via cavitation causes the popping/cracking sound.
There are various studies on the subject.
Of note is a 50 year case study of a doctor documenting himself after cracking his knuckles everyday. The doctor did not end up with arthritis.
One of the studies above showed that the forces involved with the joint manipulation may have forces that exceed the force needed for articular damage. However, as a whole the evidence points to no increases in arthritis.
Another study indicated that knuckle cracking correlates with joint swelling and grip strength loss; however, other traits such as manual labor, biting of the nails, smoking, and drinking alcohol also did as well. So there may be potential confounding factors. None of the other studies concluded this. There may be some logic to this in that people with certain personality traits, overall bad habits, and lots of stress may be predisposed to poorer recovery or ligamental laxity. I do not think this is something to worry about though.
The swelling and loss of grip strength is particularly interesting though. Everyone has different genes for how tight the articular capsules of their joints and ligaments are. If you have joints that are particularly lax (meaning "double jointed" in layman terms), it may not be a good idea to crack your knuckles. This can also vary depending on gender. Females that are pregnant will have more of the hormone relaxin flowing in their body (o get ready to give birth). Thus, ligamental laxity may increase. Therefore, it may not be a good idea to erack the knuckles if you are pregnant.
Lax joints are associated with increases in orthopedic injuries and lower strength. Since the joints themselves are a bit more unstable because of the loosene e tissue, the body cannot is of the conne generate as much force lest it injure itself. Therefore, potentially increasing this joint laxity may be a problem.
This is common in sports with excessive flexibility work such as rhythmic gymnastics where the articular joint capsules can be stretched out significantly. As a precautionary measure if you have looser joints I would avoid cracking them just in case it may present problems down the line. This is especially true if you notice that your joints are being "stretched out" so that they can move further and further each time you crack them.
Obviously, laxity in joints can be compensated with proper strength work to an extent. Therefore, if you are double joint or have general looseness, it may be a good idea to do structured strength work just because it will help protect you against injury.
Finally, erepitus can be present where there is degeneration in the joint, and it cracks inadvertently. If you suspect you have something similar, it is obviously best not to crack them.
In general, it is easy to loosen something. However, it is hard to try to tighten something. Therefore, if you are worried than do not do it. However, I have seen no significant evidence that says cracking negatively affects joints in the long term
The common answer to joint clicking is that if it is painless it is finc. I agree with this assessment especially if you have always had it
For example, people with more lax joints as described above may have always had issues with clicking albeit not painful clicking. This is fine. The general solution with lax joints and clicking in the knees, hips, elbows, and shoulders is proper strength work. Keeping the joints strong and balanced with proper biomechanical movement will stave off potential injuries.
However, if you have not always had joint clicking, and it is acute onset from particular sports, weightlifting, or other activities I would reexamine the activity to ensure that the clicking may not devolve into something insidious
In most cases, injuries can be boiled down to issues of
When these aspecis are compromised especially the limbs — ankles, knees, hips, wrists, elbows, shoulders — there is potential for clicking and popping to begin and potentially become malicious.
We will look at the knee for an example since it is the most common source of clicking (shoulder coming in at a close second). The knee is special because it has two extra pieces of articular cartilage, the menisci, in between the femur and tibia. Thus, impinging of this tissue during movement makes clicking is fairly common occurrence if something is off with biomechanics. Clicking is not always insidious though, so do not be afraid if you have always had it.
In most cases the neural factors of posture and movement biomechanics contribute heavily to the deficiencies that develop in mobilty and many muscle imbalances that rise. It st development of such imbalances or limitations in mobility that have the potential to cause clicking within the knee to devolve into painful wear on the cartilage.
For example, one of the common semi-pathologies that develops in a culture with desk jobs and sitting is the imbalance of quadriceps dominance and hamstring weakness.
Such imbalances give rise to problems with the articulation of the joint itself. When synovial joints move against each other they must simultaneously glide and roll to function correctly.
When mobility is limited by tight muscles and there are imbalances within antagonistic muscles, the biomechanics of the movement are altered.
Particularly with the knee if the hamstring do not engage correctly during walking or squatting motions, there is likely an excessive anterior glide of the femur on the tibia. This places a much larger torque on the patellofemoral complex. This is bad for multiple reasons:
Excessive anterior gliding of the femur may start to impinge the anterior portions of both the medial and lateral menisci which cause clicking. This wears down the meniseus and articular cartilage faster contributing to osteoarthriis.
Excessive anterior gliding of the femur puts more strain on the ligaments of the knee.
The increased torque on the patellofemoral complex causes the quads to become much more active thus aggravating the imbalance of the quadriceps: ing strength ratio.
The increased torque on the patellofemoral complex may lead to maltracking.
These problems are not just manifestations of the whole knee complex. Weakness and decreased mobility at the ankles and hips may also contribute to dysfunctions at the knee. Same with the shoulder, elbows, and wrists.
This is why teaching proper posture and biomechanics while improving mobility and imbalances is so important. For example, we can use box squatting — focusing on sitting back properly to engage the hamstrings and glutes — to help negate quad dominance. This occurs because sitting back shifls the weight distribution of the squat towards the heels will keep the shins upright thus decreasing the torque on the patellofemoral complex and the engagement of the hamstrings will help negate excessive anterior gliding of the femur. This should make the knee joint function properly, and it teaches proper human movement.
Earlier 1 listed the shoulder as the second most common site of clicking. While it does not have two extra picces of cartilage as the knee, it has the most mobility and range of motion as any of the joints in the body. Thus, it is very easily destabilized by problems with posture, biomechanics, mobility, and muscle imbalances.
Clicking with limited mobility in the shoulder can be eliminated in some cases if tight muscles are the issue. For example, if the clicking feels more "anterior" in the shoulder that can mean that the muscles on the front of the shoulder or the joint capsule itself is tight. Thus, stretching the muscles and joint capsule on the front of the shoulder may help to eliminate the clicking altogether. This is because stretching will help decrease the limitation on posterior glide of the humerus on the labrum (c.g. the anterior tightness is keeping it forward and not letting it go posterior) which will make it move better. This is one of the big things to note especially if your shoulders are particular immobile and you start to develop clicking sounds. Stretching may help solve the problem altogether.
In conclusion, if you know you are having recent onset clicking issues as well as problems with posture, biomechanics, mobility and muscle imbalances you may have an insidious onset of clicking that may devolve into worse problems.
In many condition significant and even eliminating cartilage clicking. This may be the case even in people that have had clicking all their lives from loose joints.
ses correct the imbalances with proper strength and mobility work should improve the
If you have tissue that is rubbing and snapping over tissue. This signifies an injury condition.
This occurs where tissues are not moving where they are supposed to be such as IT band snapping syndrome and triceps snapping syndrome. There arc other similar problems like nerve and tendon snapping/popping that may occur in different parts of the body.
In all of these cases, there is likely some problems related to posture, biomechanical, mobility and muscle imbalances. This is not unlike the clicking scenario.
The "quick" fix to eliminate the pain and snapping quickly is to loose up the tissues with soft tissue massage and anti-inflammatory drugs. However, to eliminate the problem entirely all of the factors that contribute to their development from the four atributes (posture, biomechanics, mobility and muscle imbalances) must be examined and corrected.
If connective tissue that was holding say the triceps tendon in place is gone from an accident then correcting the four factors may not help. This may be something you have to talk to your doctor about to consider if it needs surgery.
Likewise, crunching tends to represent an injury condition as well where the articular cartilage is not working properly or there is already damage where it is mashing into each other. It is best to get this checked out by a doctor.
If you have no idea how to correctly evaluate yourself and perform correct soft tissue work then go see a health professional.
Joint eracking and popping does not cause increased incidence of arthrits.
If you have lax joints, however, you may want to avoid this just in case it may present problems later due to potential destabilization of the joint. Focus on increasing strength of the muscle/tendons that connect there. This is especially true if you notice the laxity is increasing over time.
Clicking without pain is in general fine, especially if it has been there all of the time.
Sometimes insidious onset of clicking may devolve into potential problems later on. Correct assessment of posture, biomechanics, mobility and muscle imbalances should be initiated through proper strength, mobility, and soft tissue work.
Snapping and crunching signifies injury conditions. Like clicking proper care must be undertaken by 2 a doctor of physical therap
Most of the cramping you may experience will be during active flexibility exercises such as compression exercises.
For example, the active straddle compression or L-sit work may cause cramping in the quadriceps, hip flexors, or abdominal muscles. Likewise, upper level progressions of the V-sit and manna may cause cramping in the triceps as well as the aforementioned areas.
When muscles are moved into a short range of motion and contracted (active insufficiency), they are ely to cramp. A sustained muscle contraction cuts off oxygen availability and the muscles cramp due to lack of ATP. Since ATP is used to release myosin heads from actin, and used to pump caleium back into the sarcoplasmic reticulum it creates sustained intense contractions. Also, since there are a lot of actin- myosin overlapping in a highly contracted muscle it will increase the propensity for more of the heads to grab on and contract. People that are inflexible usually have tight musculature and lots of scar tissue already and are thus "predisposed" to poorer blood flow and easier cramping.
Foam rolling, massage, and static stretching are musts. However, this phenomena goes away if you continue practicing just like soreness tends to go away if you continually exercise. Thus, cramping is fairly normal to occur in the beginning, but will get better and go away through time so persevere.
If you are experiencing cramping not during exercise then this may be a different issue altogether and you should check other factors to make sure you are getting properly hydrated and enough nutrients or vitamins such as magnesium, sodium, and potassium in your diet
In particular, magnesium is a key player in muscle relaxation so it is important to get enough of it since the modern diet is deficient in this particular mineral.
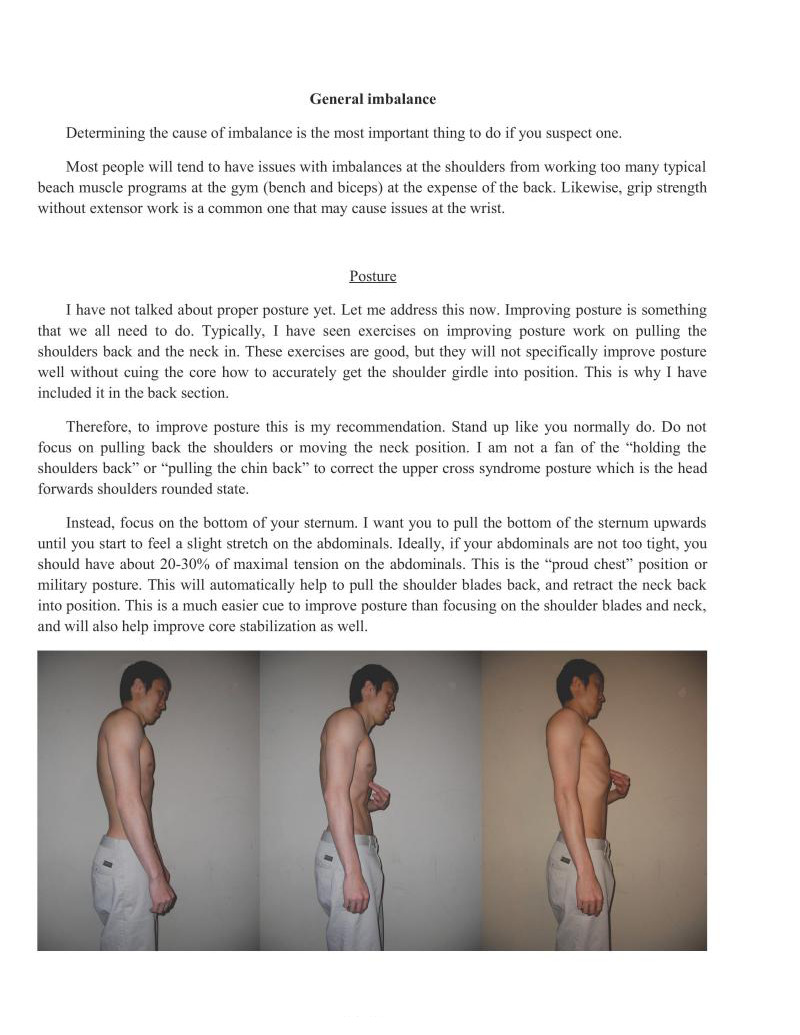
Determining the cause of imbalance is the most important thing to do if you suspect one.
Most people will tend to have issues with imbalances a the shoulders from working too many typical beach muscle programs at the gym (bench and biceps) at the expense of the back. Likewise, grip strength without extensor work is a common one that may cause issues at the wr
I have not talked about proper posture yet. Let me address this now. Improving posture is something that we all need to do. Typically, I have seen exercises on improving posture work on pulling the shoulders back and the neck in. These exercises are good, but they will not specifically improve posture well without cuing the core how to accurately get the shoulder girdle into position. This is why I have included it in the back section.
Therefore, to improve posture this is my recommendation. Stand up like you normally do. Do not focus on pulling back the shoulders or moving the neck position. I am not a fan of the "holding the shoulders back" or "pulling the chin back" to correct the upper cross syndrome posture which is the head forwards shoulders rounded state.
Instead, focus on the bottom of your sternum. I want you to pull the bottom of the sternum upwards until you start to feel a slight stretch on the abdominals. Ideally, if your abdominals are not too tight, you should have about 20-30% of maximal tension on the abdominals. This is the "proud chest" position or military posture. This will automatically help to pull the shoulder blades back, and retract the neck back into position. This is a much easier cue to improve posture than focusing on the shoulder blades and neck, and will also help improve core stabilization as well,
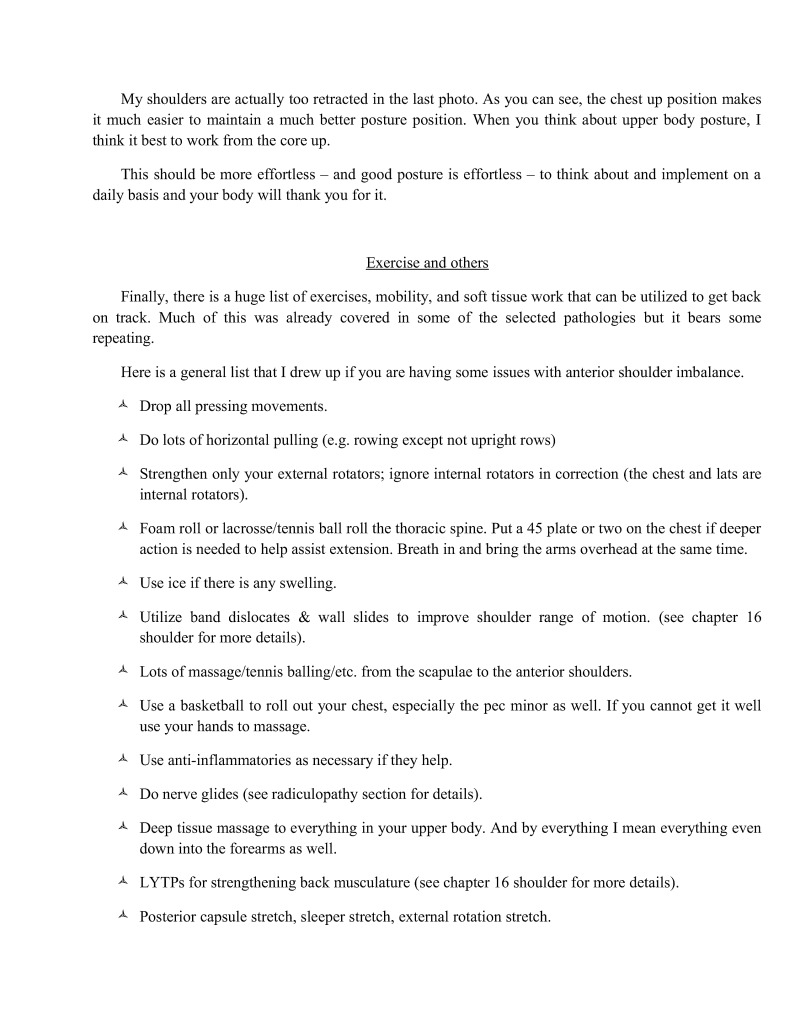
My shoulders are actually too retracted in the last photo. As you can see, the chest up position makes it much easier to maintain a much better posture position. When you think about upper body posture, I think it best to work from the core up.
This should be more effortless — and good posture is effortless — to talk about and implement on a daily basis and your body will thank you for it
Finally, there is a huge list of exercises, mobility, and soft tissue work that can be utilized to get back on track. Much of this was already covered in some of the selected pathologies but it bears some repeating.
Here is a general list that I drew up if you are having some issues with anterior shoulder imbalance.
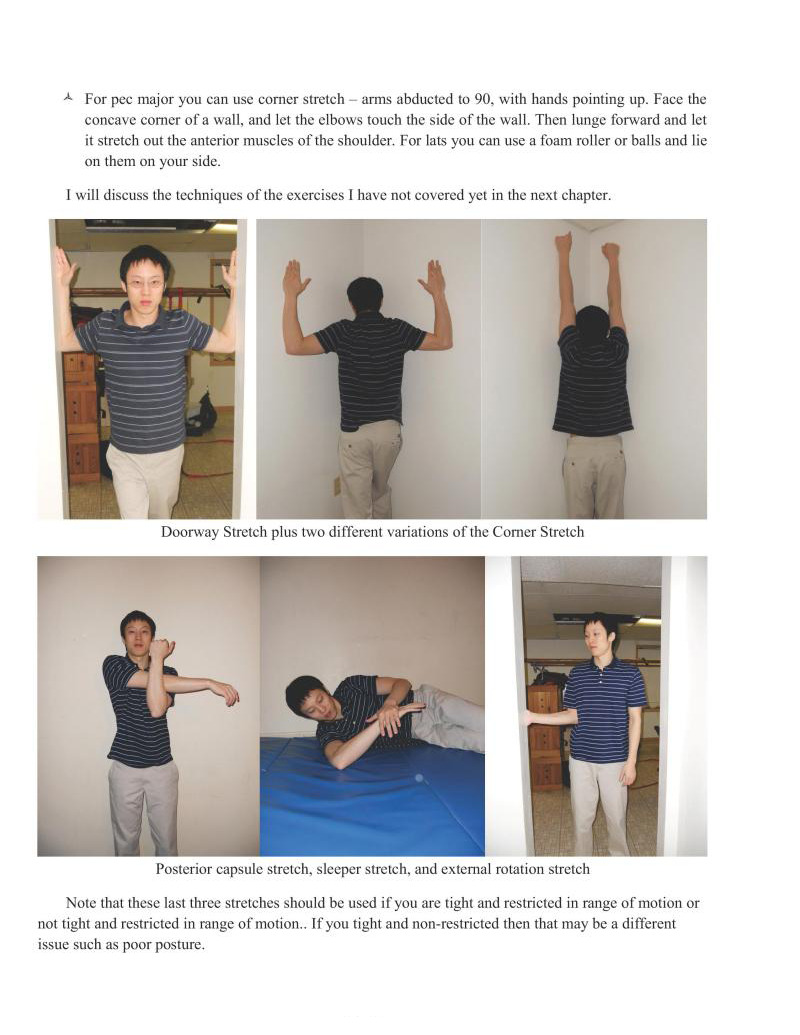
Note that these last three stretches should be used if you are tight and restricted in range of motion or not tight and restricted in range of motion... If you tight and non-restricted then that may be a different issue such as poor posture.

This chapter talked about some selected common injuries that may develop when training for bodyweight movements or skills.
Remember, this book/chapter is not meant to diagnose any injuries. If you have an injury and are unsure I would suggest again that you make an appointment with your doctor, physical therapist, or chiropractor and figure out what you are dealing with. Once you figure that out, then this chapter may be more useful to you.
Remember to keep this in mind because I will be talking about these types of injuries like they are common. If you have pain in the areas I describe just because they are common does not mean you have that specific injury. Using certain exercises or rehabilitation techniques for injuries which have not been diagnosed may actually make them worse. Again, if you have any sort of pain get it checked out by a qualified medical professional so you can know what you are dealing with.
The contents in this chapter is meant to be informative and any use of corrective measures should be done at your own risk.
Previous Chapter ... ... Next Chapter