Previous Chapter ... ... Next Chapter
I think that injuries are best thought of in a chronological based context. What exactly are we aiming for at certain points in the injury?
Thus, we have this hicrarchy that we can use when we look at any particular injury to see what we need to focus on at that py
in time.
Determine cause of injury.
Eliminate any offending stimuli be them movement, particular exercises (pathomechanics), or other acute/chronic injury stimuli
If the pathology is known, rehabilitation must be integrated with tissue remodeling phases dependent on diagnosed pathology.
Critical points in tissue inflammatory phase:
Critical point of tissue proliferation and remodeling:
Tissue healing rates vary depending on what tissue is injured. For example, skin injuries typically heal up in a few weeks. If you had a cartilage injury or shoulder labrum repair, the proliferation and remodeling phase may last well into 3-4 months down the line. Functional activities such as throwing will not be prescribed before that amount of time with patients in physical therapy.
Thus, it is very important to understand what is actually injured, and what type of protocol is needed to treat that specific injury. In every chapter of the health and injury management section I have been advocating getting injuries diagnosed so at least you know what it is even if you do not go to physical therapy for it, This is precisely the reason why.
All of the information in the previous chapters is highly generalized. For example, information in the tendonitis artiele may not apply specifically to everyone. People may have tendonitis without any extremely tight muscles. Ice may help better than heat. Maybe neither modality will help at all. Massage may or may not be uscful.
If you do utilize the general information contained within the previous chapters you need to listen to your body.
If so, modify prehabilitation and rehabilitation as necessary.
In conclusion, use your critical thinking abilities. Do not just do something because I said it or someone else suggested something. When in doubt, see a medical professional.
Here is a chart on what particularly works well for exercise regarding injury conditions. It is created from my physical therapy notes.
As you can see, there is a bit of difference in regards to the muscular recommendations from earlier in the book. This is because there is some conflicting evidence in the literature on what actually works the best for what in particular. For example, some studies have noted that for strength beginners tend to respond best to around 60% 1 RM instead of the typical 80-90% RM which falls around the 4-8 repetition range.
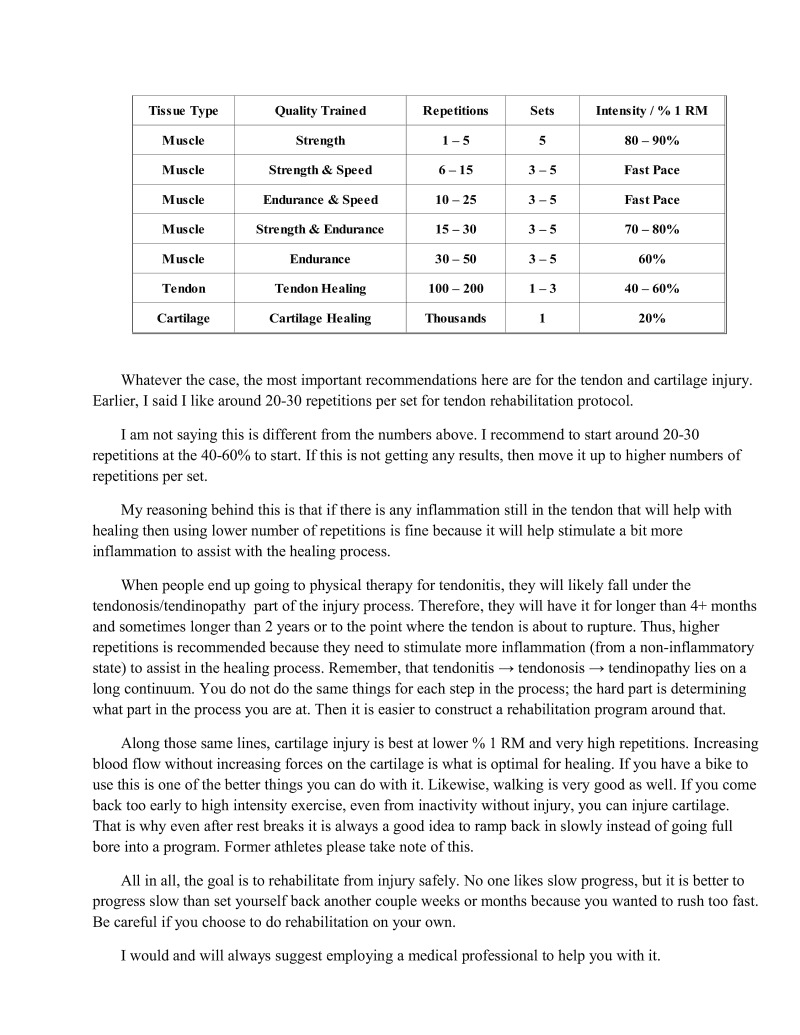
Whatever the case, the most important recommendations here are for the tendon and cartilage injury. Earlier, I said I like around 20-30 repetitions per set for tendon rehabilitation protocol.
I am not saying this is different from the numbers above. I recommend to start around 20-30 repetitions at the 40-60% to start. If this is not getting any results, then move it up to higher numbers of repetitions per set.
My reasoning behind this is that if there is any inflammation still in the tendon that will help with healing then using lower number of repetitions is fine because it will help stimulate a bit more flammation to assist with the healing process.
When people end up going to physical therapy for tendonitis, they will likely fall under the tendonosis/tendinopathy part of the injury process. Therefore, they will have it for longer than 4+ months and sometimes longer than 2 years or to the point where the tendon is about to rupture. Thus, higher repetitions is recommended because they need to stimulate more inflammation (from a non-inflammatory state) to assist i the healing process. Remember, that tendonitis — tendonosis — tendinopathy lies on a Tong continuurn. You do not do the same things for each step in the process; the hard part is determining what part in the process you are at. Then it is easier to construct a rehabilitation program around that.
Along those same lines, cartilage injury is best at lower % 1 RM and very high repetitions. Increasing blood flow without increasing forces on the cartilage is what is optimal for healing. If you have a bike to use this is one of the better things you can do with it. Likewise, walking is very good as well. If you come back too early to high intensity exercise, even from inactivity without injury, you can injure cartilage. That is why even after rest breaks it is always a good idea to ramp back in slowly instead of going full bore into a program. Former athletes please take note of this.
All in all, the goal is to rehabilitate from injury safely. No one likes slow progress, but it is better to progress slow than set yourself back another couple weeks or months because you wanted to rush too fast. Be careful if you choose to do rehabilitation on your own.
I would and will always suggest employing a medical professional to help you with it.
In prior chapters, I have stated two generalizations about pain:
Never work through pain.
Pain can be used as an indicator during rehabilitation when knowing something is too much.
These are definitely true most of the time. However, when we are dealing with more severe injuries these statements have limitations. I assume that most people will not be rehabilitating any type of catastrophic injury by themselves like a meniscus tear, or shoulder labrum tear (c.g. SLAP lesion), or any other potential injuries like that. However, I am going to talk about it for the sake of it being critical information about rehabilitation in general.
Connective tissue that is ruptured and repaired such as tendons, cartilage, ligaments, etc. have much longer healing times than skin, muscle tissue, etc. because of increased vascularization in the latter tissues. Therefore, even if there is no pain present in these types of tissues, there may be potential range of motion or strength restrictions that doctors and physical therapists may place on the patients. Hence, limiting range of motion or strength is obviously a good idea — you do not want to be creating and/or exacerbating the inflammatory healing process of these tissues when they are weak
As I stated near the end of chapter 14, sometimes it may take upwards of 2 months before active range of motion is allowed, and 34 months before any significant functional activities are performed with particular cartilage injuries because of the slow healing rates.
Thus, pain is good as a general guide for most non-significant injuries. However, once you have a catastrophic injury or a surgery, things may change. Likewise, during physical therapy regaining range of motion, strength, or functional mobility may cause pain. In general, it is not good to work through pain; however, sometimes it is necessary during a physician or physical therapist supervised rehabilitation process.
I just want to get this important information out there. If you are having any potential issues always consult your physician or physical therapist about why you may or may not be performing certain things at different points in your rehabilitation. They should be able to tell you and justify it with a physiological rationale. If they cannot then that may be a problem.
Generally speaking, there is a hierarchy that we want to climb as we rehabilitate from an injury:
After an acute or chronic injury, we want to assure that there is stability there. That is to say we want to make sure the joint or tissues are protected. For example, if we had a fracture we want to ensure stability of that bone so it can heal correctly. Hence, we put it in a cast. Another example would be with a severe sprain. Sometimes we need to wear a boot if it is at the ankle, a knee sleeve if it is as at the knee, or asoft aircast if it is at the wrist.
As soon as the injured tissues are healed enough, the next thing we wan to do is initiate exercise to increase range of motion. If we run with a sprained ankle example, this is where we will start inserting stretching exerises for range of motion and mobility exercises taking the foot through non-painful ranges of motion.
After increasing the passive range of motion, the next concept to look at is to strengthen it through that range of motion in a controlled fashion. This is where the controlled concentrics with slow eccentrics comes in. We are aiming to foster stability (through the strength or endurance training) in movement.
Typically, we will start out with high repetitions of around at least 20-30 if not more to ensure that the weight is light cnough that it does not cause any damage, and to ensure we work all of the particular muscles we are aiming for in an endurance fashion. We aim for endurance at this point because endurance training is critical to prevent injury when the particular area is fatigued. This is why rotator cuff exercises are generally always higher repet the end of training. We never want them to fatigue to the point where they will give out on us.
jon exercises since they are easily injured if something goes wrong near
Finally, we have explosive movements which are what we should be strive for athletically.
Lam sure most of you have heard of the stability and mobility continuum where alternating segments of the body seem to have been " for one or the other. For instance:
As you can see, the feet, knees, lumbar spine, cervical spine, scapula, elbows, and palms all tend to be built for stability. This means that if they gain too much range of motion without enough strength and stability bad things start to happen. The most prevalent sources of pain when there is excessive range of motion or weakness tend to occur at the knees and low back. However, other detrimental effects on certain structures are seen when they become weak or with poor posture such as in the feet (fla feet, etc.) or cervical spine (neck pain, radiculopathies, etc.) or scapula (the shoulder cannot move correctly). Since all of these intertwine with the mobility segments, we see a lot of interaction between the two which I will talk about next.
The joints that tend to be built for mobility are the toes, ankles, hips, thoracic spine, shoulder/glenohumeral joint, wrists, and fingers. Obviously, most of these are relatively straight forward as can be seen in many fundamental movements such as running, squatting, and reaching tasks.
The only real confusing one for most people to understand is the T-spine. Although the T-spine does not have very great extension, it does have a fair amount of range of motion to bend forward and rotate from side to side. Most of the problems creep up when the T-spine becomes immobilized due to poor posture, tight muscles, or other pathological issues. When one "segment" has decreased mobility, the body compensates by obtaining mobility from other segments.
Usually with a restricted T-spine you will see that the lumbar spine tends to take up a lot of the. mobility slack. This is one of the things that contributes a lot to the development of low back pain due to increased range of motion without increased strength to stabilize. Likewise, a restricted T-spine will not allow the seapula to move along the ribs well which will also restrict shoulder range of motion overhead and alter glenohumeral mechanics possibly causing shoulder pain. Additionally, a restricted T-spine will also contribute to a shoulders forward and head forward posture.
Therefore, it is important to know why we are developing range of motion in certain places, and why we are trying to develop strength in others. In some cases, we want to do both. More range of motion makes something less stable if not strengthened, so strengthening will help prevent injury.
This is why low back pain rehabilitation may focus on improving core activation and strength. However, a competent physical therapist will also look at issues regarding the thoracic spine, hips, and if indicate other more distal joints away from the back. In some cases, foot issues can cause low back pain. Upper cervical issues in other cases may cause widespread issues all along the body because the body will compensate to keep the eyes and equilibrium of the body level
Either way, do not just stretch or strengthen blindly. If you have no reason to gain range of motion then simply do not stretch; just maintain mobility at that particular joint. Bodyweight movements in particular require a large amount of range of motion at the hips, T-spine, shoulders, and wrists. Therefore, when coming back from injuries it is important to focus on these areas in particular.
Strength tends to always be a good thing if imbalances are not created. Thus, strength is a quality we will almost always want to develop across the whole body at every joint. This is true of not just bodyweight exercises but all movements and across all disciplines. Typically, the strong athlete is the better athlete (though there are exceptions).
Remember how it is possible if you stretch excessively that you will be sore the next day?
This brings me to the statement that I think people tend to forget: stretching is eccentric exercise!
When we lengthen a muscle, the muscle spindles in our muscles tell the body that the length is getting too long and will be dangerous. Thus, the motor neurons in the spine will be told to contract the muscle to try to stop the lengthening of the muscle. Yes, this contraction is indeed a contractile form of exercise albeit an involuntary one.
Regardless, as we stretch out the muscle more we lengthen it against contraction — it is just like eccentric exercise. Lengthening a muscle it repeatedly against contractions will induce microtearing of the muscle. This is why we get the soreness both from eccentric exercise and from stretching.
The main point I am trying to make with this is that if you have an injury and you cannot workout that stretching is useful in rehabilitation in both correcting imbalances and protecting and strengthening muscles against atrophy.
From my experience, when stretching is combined with a good sleep schedule and diet, you will likely not lose any of the muscle gains you have acquired if you are on an off week or are rehabilitating from injury. It is definitely a very useful concept to keep in mind, especially if you need to work on your
Having goals for injuries is important. All physical therapist must have functional goals for their patients. It is required for insurance reimbursement and to justify what type of treatment is given. For our purposes, it gives us a time line on which we can base our rehabilitation on.
The thing about injury goals is that it is often harder to know how long it may take an injury to heal or even know how it may respond to treatment. Additionally, you may not know enough about an injury to even know how to rehabilitate it. This is why I recommend professional help almost always.
However, if you are into self treatment goals arc definitely important. Like your workouts you should know that if you are not progressing from rehabilitation session to rehabilitation session or week to week then there is something wrong. This is where the goals become important — they allow us to think about and identify what may or may not be working at getting us to our goal. They keep our motivation up. We may have (o refine and modify things in our prehabilitation and rehabilitation programs to constantly make progress.
In this sense, rehabilitation is just a lower level extension of programming for regular strength and conditioning. It is not all that different from regular training. The key learning the concepts and knowing your options if you are plateauing
In this chapter we discussed the phases and important concepts of the chronological treatment of injury. In particular, there are different phases to work on different concepts such as protection from atrophy, range of motion, strength, etc. during the inflammatory, proliferation, and remodeling phases.
We also learned more on the particular loading, repetitions, sets, and volume of rehabilitating from specific injuries. Each injury needs to be taken in particular context of its severity and interference with normal function.
We looked at pain and its application during the rehabilitation phase. While we know that generally we should not work through pain, it depends a lot on the particular injury. Thus, if we have any doubt about rehabilitation we should consult a professional.
We examined the concepts of range of motion and strength and their relation to stability and mobility in various joints of the body and how it applies to rehabilitation. In particular, we concluded that strength without imbalance is very good, and that we should only increase range of motion as much as we need for particular movements or holds.
We learned that stretching is eccentric exercise. This is a very important concept in rehabilitation that many people overlook. It is useful for deterrence of atrophy and critical for helping correct tension balances during rehabilitation
Finally, we noted that injury goals are important. Make them.
Previous Chapter ... ... Next Chapter