Previous Chapter ... ... Next Chapter
Injuries are a particularly hard topic to address since there is no one-size-fits-all prescription to nurse someone back to health. Everyone responds differendy to treatments and has different recovery factors to take into account, including but not limited to: nutrition, sleep schedule, general overall health, and training schedule. It is absolutely crucial to receive individual care for your specific injury. Certain issues absolutely require a visit to an orthopedic sports doctor or physical therapist.
With this in mind, understand that the information contained in chapters fifteen and sixteen reflects a generalized approach to health and injury management. Something that may work very well for one athlete may not work at all for someone else-it could even have a negative effect! Every athlete is different. A doctor or therapist will be able to examine your individual situation and prescribe rehabilitative or prehabilitative work to restare you to health. If your medical professional says something that contradicts information provided in these chapters, listen to them as they know your case!
Any information found in chapters fifteen and sixteen of Overcoming Gravity is for informational purposes only. None of this should be misconstrued as medical advice. You should always consult your medical professional before utilizing any information located herein. Self-treatment without advice from a medical professional is not recommended and is therefore at your own risk.
Everyone has heard the saying, No pain, no gain. The phrase is ubiquitous in the athletic world for pushing through pain. Some coaches-typically at the high school level and below-believe in this saying unconditionally. Let's distinguish between "the burn" pain, and soreness in order to get a better understanding of the concepts these terms represent.
The pain you feel during exercise when your muscles start to "burn" or after exercise is completed does not typically have a negative impact on your body, except in rare situations where is becomes excessive and you continue to push through it. A certain amount of stress on the muscles helps to force anaerobic adaptations in the muscles, a positive goal. This type of "pain" is not an injury risk.
On the other hand, delayed onset muscle soreness (DOMS) generally occurs approximately 24 hours after exercise and can last 48-72 hours. In extreme cases, it can last 7-10 days. It typically happens to trained athletes coming back from a layoff DOMS generally occurs when you (1) try new exercises, (2) increase volume or frequency, or (3) perform excessive amounts of eccentric components of exercises.
Your body is able to progress in both strength and hypertrophy without having to go through the pain of soreness or the bum. Even if you do feel sore, know that as long as you are increasing your strength, gaining musclemass, or meeting any of your goals you do not have to modify your routine. If you are not progressing, then it is time to make a strategic change of some sort-even if you are not experiencing any soreness.
Laying out some guidelines for training while sore is a good idea, as people new to training often do not realize the difference between pain and soreness and do not know when they should continue or cease exercising. Here are the guidelines:
cases, the soreness is probably hindering your workouts. Increase your frequency to 3x per week full-body and the soreness will likely dissipate.
Whether you see it as positive or negative, soreness is not something to worry about, as you can make progress with or without it. Generally, it will be more of an annoyance. If you plan on performing a high-volume workout or a routine with a lot of eccentric movements, you can expect to be sore afterward.
Pain is different. However, chasing pain or a lack of pain is not good. The best concept to understand pain in exercise is the concept of aggravating exercises. The reason why pain is less important than aggravating exercises is important. Sometimes if there is pain, an injury may feel and move better after exercise. Sometimes if there is no pain, an injury may get more stiff and worse. Hence, removing aggravating exercises is more important than trying to use pain as a guide. If there is pain, but exercises lessen the pain and improve the injury then keep those. Pain is one factor, but it is not the most important factor in determining whether to use exercises far rehabilitation or not.
Far specific advice on whether or not to work through pain, contact your medical professional. A book cannot diagnose you or correct your injuries. You can only learn the factors that affect propensity far injury, learn to integrate these principles far prehabilitation, and learn how to work around injuries in a routine.
There are four main factors that contribute to the integrity and health of tissues of the human body:
These factors all interact with one another. Posture and biomechanics represent the neural control of the central nervous system in its interaction with the environment. Posture is the static presentation of the body in space, and biomechanics are the dynamic element of movement. We receive feedback from our senses via these pathways in two ways. Proprioceptive feedback from static elements, and kinesthetic feedback from moving elements. Proprioceptive feedback is being able to sense where the body is in space, and kinesthetic feedback is the ability to sense various movements in space. The brain and its neurological system control the body, and each of these neural elements exerts influence on musculoskeletal structures.
Biomechanics effect constant recalculations of the nervous system as the environment changes. This is why exercises are the best way to teach the body how to move and work correctly. Resistance exercise is also an effective way to train the nervous system and strengthen the muscles. Maintaining proper technique in an exercise significantly reduces the propensity far injury after the body begins to become fatigued. The rest of the factors all apply broadly to biomechanical movement.
If you have ever been to physical therapy, particularly far back pain, you already know that many of the exercises prescribed are those that work on stability; in effect, re-teaching fundamental movements like those you see babies learning from birth to three years old. As we grow up, our bodies naturally learn movements
that our nervous systems reinforce. However, our culture is one of schools and desk jobs, causing us to "practice" body positions that make us lose our ability to move effectively, thus increasing propensity far injury. Becoming more proficient with rolling, crawling, squatting, and other fundamental movements that our bodies learned when we were younger will drastically decrease propensity far injury due to the body's inherent carryover effect from simple to more complex movements.
Posture or good body alignment provides a platform to optimize the ability of the musculoskeletal structures to apply and dissipate force when called upan during movement. Studies have shown that bad posture is not always correlated with pain. In other words, there is not always a structural problem in the body where there is pain. MRI studies have shown that 20-50% of healthy, pain-free populations may yet have bulging discs, herniated discs, stenosis (narrowing of a passage that nerves run through), and other degenerative conditions. They have these conditions, even though they do not have pain. Despite these studies, from a health and wellness perspective, good body alignment is a relevant factor to quality movement which may indirectly decrease propensity far injury. This is why we want to take a look at good posture.
Sitting with your shoulders hunched forward (colloquially "caveman posture") puts your shoulders in an unstable position by changing the length and tension relationships of the muscles. This is prevalent among people who perform desk jobs or work in front of a computer far hours at a time and it causes all kinds of problems. There is the increased propensity far impingement due to internal rotation of the shoulder that leads to decreased space under the acromion. There is increased risk of anterior instability that may lead to subluxation or dislocation due to posterior shoulder weakness. There is increased stress on the at joint as it moves into the overhead position, which can negatively affect overhead work like handstands. These are only a few examples of increased propensity far injury due to poor posture.
Posture also affects your thoughts and your decision-making. Those who stand taller tend to be more confldent and decisive. They are more esteemed by peers far leadership and their voice is given more weight.
It is also better far breathing and having a calm mindset in stressful situations. Your body is trained by the things you do continually. If you teach your body to do negative things, it will learn these things and adjust accordingly-leading to injuries, poor posture, and poor movements. Therefore, prehabilitation and rehabilitative protocol must continually focus on both biomechanics and re-teachingproper posture. Re-teaching your body may require more than simply a few weeks or months of constant diligence to correct problem areas. This isnot achore, but an additionalstep to improve your overall health and performance.
Mobility is the interaction of the voluntary muscles in their range of motion taking into account how posture and biomechanics affect movement. Kinesthetic feedback is provided to the central nervous system via muscle spindles, which regulate muscle length. Muscle spindles are located in the muscles themselves, while the control system far these muscle spindles is gamma motor neurons. Passive tension is generated when muscles are taken to the edge of their range of motion. Additional muscle length-tension relationships are comprised of kinesthetic feedback to the central nervous system via the golgi tendon organs.
These regulate muscle tension and the ability to voluntarily output force. Golgi tendon organs are located at the muscle-tendon junction. Both of these feedback systems are essential to regulate your posture and biomechanics.
Posture, mobility, and the manner in which force is applied all affect how you execute a technique or movement. It is important to focus on these things to build a solid foundation far quality movements. In
terms of managing injuries, an organized approach is best. If you do get injured, use this four-step approach to work your way back to performing a normal routine.
Having goals for addressing injuries is important. All physical therapists should have functional goals for their patients. This is required not only for insurance reimbursement, but to warrant the type of treatment that is given. For our purposes, goals give us a timeline. Generally, a medical professional is required to help you set your injury goals because you often do not know how an injury will respond to treatment and how long it will take to heal. You may not even know enough aboue an injury to know how to rehabilitate it. Do not hesitate to consult a medical professional to come up with goals for your injury-the following guidelines are for informational purposes only.
Goals force you to idencify what may or may not be working, and they also keep you motivated. As with your workouts, you should know that something is wrong if you are not progressing from one rehabilitation session to the next on a weekly basis. You may have to make adjustments to your rehabilitation or prehabilitation program to continually make progress in addressing an injury.
In this sense, rehabilitation is a lower-level extension of programming for regular strength and conditioning. It is not that different from regular training. The key is learning the concepts and knowing your options if you are plateauing. Keep in mind that the injured area is sensitive and prone to re-injury. Careful care muse be given to an injured body pare.
The healing cascade is a normal process of body tissue. It occurs naturally, given enough time. The most prevalent example is with the skin, but all tissues respond similarly when injured-even the brain. The process is predictable and divided into the following three stages:
It is important to realize that the healing cascade is how all body tissues mature to some extent. One of the fundamentals of workoues is that exercise damages muscle cells. Muscles become inflamed and the immune syscem cleans up the damage. There is proliferation of new muscle cells or satellite cells to repair the damage, and new contractile fibers are laid down. The muscle then matures and remodels to become bigger and stronger.
Another example is that of calluses on the hand. Stress is placed on your tissues when you lift heavy weights or hang onto the pull-up bar to the extent that your hand starts burning and hurting. Your tissues
then become inflamed and begin the process of healing. Your skin cells proliferate and multiply, and they will finally mature and remodel into a callus.
There are problems that can occur with "too much, too soon." Aggravation of an inflamed area can result in blisters, opening of wounds, scarring, and re-injury. These are so common that you should be able to apply this understanding to your prehabilitation and rehabilitation.
Injuries are best thought of in chronological context. The following timeline can be used to aid you in knowing what to focus on, depending on where you are in the healing process of an injury.
Tissue healing rates vary depending on which tissue is injured. Skin injuries typically heal in a few weeks, but if you have a cartilage injury or shoulder labrum repair, the proliferation and remodeling phase may last three to
four months since these types of cells heal slowly due to limited blood supply. Functional activities like throwing will not be approved for someone undergoing physical therapy before that amount of time has elapsed.
It is very important to understand what is actually injured and what type of protocol is needed to treat that specific injury. This is the importance of a professional diagnosis and treatment planfrom a medica/ professionall Medical diagnosis is essential even if you do not need to go to physical therapy and can selftreat your injury. In the context of prehabilitation and rehabilitation, you should be asking yourself these questions:
Use your critical thinking abilities. Do not do something just because it was suggested to you. When in doubt, see a medical professional.
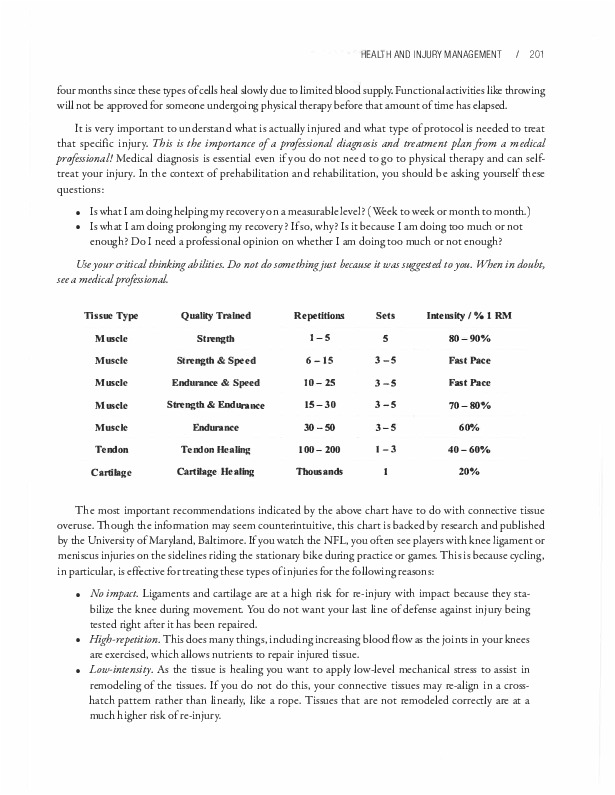
Tusue Type Quallty Trained Repetitions Sets Intensity / ¾ 1 RM Muscle Strength 1-S 5 80-90% Muscle Strength & Speed 6-15 3-S FastPace Muscle Endurance & Speed 10-25 3-S FastPace Muscle Strength & Endurance 15-30 3-S 70-80% Muscle Endurance 30-50 3-5 60% Tendon Tendon HeaUng 100-200 1-3 40-60% Cartilage Cartilage Healing Thousands 1 20%
The most important recommendations indicated by the above chart have to do with connective tissue overuse. Though the information may seem counter-intuitive, this chart is backed by research and published by the University of Maryland, Baltimore. If you watch the NFL, you often see players with knee ligament or meniscus injuries on the sidelines riding the stationary bike during practice or games. This is because cycling, in particular, is effective for treating these types of injuries for the following reasons:
There are several effective approaches for overuse prehabilitation or rehabilitation injuries. The general time frame is the same as a mesocycle, four to eight weeks. This tends to be a bit conservative for prehabilitation but is usually spot-on for rehabilitation.
These types of exercises respond well to a 2151 tempo, but any similar tempo that varies the time by one second can also work well: 1-3, 0-2, 4-6, 0-2. It is only important to have a controlled concentric component
of 1-3 seconds so as to limit the speed of the repetition in order to ensure that there is enough time to concentrate on proper technique. After a slight pause or rest at the end of the repetition, the 4-6 eccentric phase (muscle lengthening) will re-educate your nervous system to fire correctly. It will also injury-proof the tissue. End with a slight pause or rest at the end of the repetition.
The eccentric tends to be the most useful component in treating any type of pain or injury, especially in prehabilitation and rehabilitation of tendonitis and strains. The eccentric component of exercise causes muscle damage which creates an inflammatory response which is necessary for healing, especially in chronic injuries. The eccentric component also provides sustained, low-intensity stress for remodeling. High repetitions along with muscle contraction help to force blood in and out of the particular areas that need it.
The eccentric component may very well be critical for re-teaching your body to correctly activate its museles once again, since eccentrics preferentially activate fast-twitch fibers. After a sprained ankle, your body will experience pain, causing your nervous system to sense a threat - which in turn causes your muscles to spasm and tighten to protect the injured area. Eccentrics re-train your nervous system to decrease the threat response and increase motor control again. If you have injured a particular area, you may experience shakiness when trying to control a movement once you begin to perform rehabilitation work. You can correct this with a uniform-speed eccentric movement.
In the physical therapy clinic, eccentrics have also been used to increase flexibility. Patients with frozen shoulders or impaired internal/external rotation have improved 20-30 degrees in range of motion in a single session using not-to-failure slow eccentric motions. The reason for this may be that eccentric movement allows the nervous system to decrease the threat response and re-teach neuromuscular control. The decreased threat response is manifested in a desensitization of gamma motor neurons, which control muscle spindles, which control muscle tension at the edge of the range of motion, usually increasing it. If decreasing your threat response decreases the sensitivity of the muscle spindles, you should be able to move your muscles into a new range of motion.
The theory works well in practice. Slow eccentrics through the range of motion to the edge of the range of motion can be used effectively to gain flexibility or increase range of motion, especially after injury. Aim for a general, systematic approach when addressing a specific area. Here is a typical order of progression for this:
Here are specific details for each of these phases. Adjustments can be made depending on how the area heals.
When executing prehabilitation exercises, there are some additional factors you should take into consideration. Adherence to these items will speed your recovery, but keep in mind that there are still physiological limitations of time for healing to fully take place. Here are the factors to consider:
Pain is another big inhibitor of muscle function. Whenever your body senses a noxious stimulus, it sends feedback to the motor cortex to inhibit force production. In other words, if you punch someone in the arm and then make them lift weights, their capabilities will be inhibited even if there is not significant damage to their muscles. Your body has natural limiters on the muscle via golgi tendon organs. They limit motor drive if there is pain present.
If you have suffered a catastrophic injury, the amount of time it will take to recover can be estimated by the number of letters in the name of the tissue that is injured. This is fairly easy to remember and gives a
good approximation. For example, a torn ligament will take approximately 8 months (ligament = 8 letters) to rehabilitate properly. Your other tissues are cartilage (9), bone (4), muscle (6), and tendon (6). These figures are used only for catastrophic injuries. Strengthening your tissues to the point where you can exercise again should only take a fraction of this time.
Your overall goal is to reach the point where you can again perform the exercises on your original workout plan. You must progress from low-intensity to high-intensity repetitions of an exercise. Taking a month to get back to full workload is going to be typical for a minimal to moderate injury (around a Grade I strain or two to three months of tendonitis). Decreasing the volume in your routine for a month will allow your tissues to calm down and recover properly. Scale accordingly.
For minimal injuries, it will take a quarter to half of the time that the injury has been present. If the injury has !asted for four months, it will likely take four to eight weeks to reach full health. This is dependent upon individual recovery factors-diet, sleep quality, stress levels, abilicy to rehabilitate without pain, how your body responds, and more.
This is an extremely conservative protocol, but it is wise to spend a little extra time now so the same injury will be less likely to re-occur. When in doubt, it is always best to err on the conservative side when it comes to volume. You can always increase the volume if needed, but if you attempt to do too much, it is easy to re-injure yourself. Talk to your medical professional and take it slow.
There has been alot of discussion and debate in recent times about a RICE vs. MEAT approach. The following is for informational purposes only; calk to your medical professional before using any of these methods. Here are the deflnitions of the two acronyms.
RICE
MEAT

The RICE approach is the traditional model for injury treatment. The MEAT approach is an alternative model that is basically physical therapy rehabilitation in disguise. It is important to note that in the MEAT approach, physical therapy is indicated from day one or even day zero. Have a knee replacement? Sprained your ankle? The studies show that earlier you can begin physical therapy, the better. The only cases which are exempted from this are surgeries like ligament or tendon repairs that require anchors or sutures to heal a bit before beginning physical therapy, and any injury that is given a non-weight bearing status.
The RICE approach is rarely used anymore, even for acute injuries like a sprained ankle (assuming there are no catastrophic issues like torn ligaments or broken bones). Rest is obviously not good for a sprained ankle. You want as much early movement as you can get within your pain tolerance level. Slow range of motionmovement will actually decrease your pain in many cases. lmmobilizing the area leads to much longer recovery times because your muscles begin to sciffen up and motor control qualicy decreases. The use of it. is hocly debaced. In practice, if there is no swelling taking place, it. is unnecessary. If there is swelling, compression is actually more effective than it.. it. is really only useful for dulling pain, and analgesics usually work better for this. If you use compression, elevation is also unnecessary. Based on these factors, the RICE approach would seem to be outdated and inferior to the MEAT approach.
To wacch the MEAT approach in action, one need only take notice of chose athletes with severely sprained ank.les who return to jogging and running the next day when they could not put weight on it for 15-30 minutes after the sprain. For an inversion sprain (where the foot rolls inward), work into dorsiflexion (moving your toe toward your head) and eversion (out, to the side, away from your other foot). Plantarflexion (moving your toe away from your other foot) and inversion (moving the toe toward your other foot) will be painful, since that is how you sprained it. However, if you move slowly and continue to mobilize into dorsiflexion and eversion, the pain will typically begin to subside wichin ten minutes, and you may even be able to walk on it. If you remain unable to walk, continue to mobilize your ankle with light massage. You should eventually be able to walk without a limp, though your ankle and foot will be sore.
People who use the RICE model often wind up limping or needing assistance to walk, and continue to have difficulty walking for up to a week or more. On the other hand, those who begin mobilization early on, do not use it., and continue to gently mobilize the injury into the night, tend to wake the next morning feeling fine. They can walk normally and some can even jog or run. The opinion of a medical professional can not be overstated. If you use the MEAT approach without consulting a medical professional, you do so at your own risk.
Working around injuries typically involves removing aggravating exercises in your routine and replacing them with alcernative and supplemental exercises until the injury is corrected. The most important ching is that you continue to rehabilitate injuries as you work around them.
Stay in the habit of working out. lntra-limb and opposite limb exercises are tools used for maintaining strength in the joint that has been injured while you continue to normally exercise the unaffected limbs and other areas. This promotes blood circulation which facilitates healing in the areas that have been injured.

In the following example, the athlete has a right shoulder injury. It still hurts to move it, and there are doctor's orders to rest/avoid exercise with this injured body part. Here are some types of exercises you can utilize when working around the injury.
Alternative Exercises
These are the two main options. It is important to keep workingout (safely!) inarder to maintain strength and hypertrophy gains and stay in the habit of exercising regularly.
The number one reason your muscles begin to atrophy (the opposite of hypertrophy) is immobility and disuse. Atrophy caused by immobility occurs very rapidly, often as soon as a week or two after restricting a joint due to injury. Anyone who has worn a case after breaking a bone has seen how this works.
Using the example of the shoulder injury, the first thing you want to examine is whether or not you can use the rest of your arm for exercise. If so, you can counter the effects of atrophy with isolation exercises for your elbows, wrists, and fingers. If a doctor has been seen, it would be a good idea to talk to them to see if arm or forearm exercise is contraindicated during the period of immobility for the shoulder. If exercise is cleared, it is time to get busy.
This is a great time to perform specific isolation exercises for your arms like biceps curls or triceps extensions. Forearm exercises can maintain strength in your arm while your shoulder is immobile. Grip work is often a good choice as well. Exercises that use part of the shoulder muscle for stabilization should be avoided if they irritate the injury.
Using your arm and forearm muscles sends neurological output to the arm as a whole-important, because the radiating effect of neuromuscular impulses will flght atrophy. Activity from the motor neurons is very important to the health of the muscle. In fact, if one were to cut through a motor nerve or sever the spinal cord, related muscles will begin to atrophy within a matter of days. In the case of shoulder injury, you may find it harder to grip the bar during pull-ups or dips due to this effect.
You should aim to do as much light exercise or mobility work as you can without irritating the injured area. It will stimulate blood flow, thus speeding up the healing process and preventing muscle atrophy while maintaining this very important range of motion.
There are almost always ways to continue training injured limbs without making the injury worse. However, if any type of movement irritates an injured joint, this is a major red flag and you should see a medical professional immediately. If your doctor or physical therapist has given you the green light to perform rehabilitation work, but doing so is painful, consult them as well. There are some instances where it is helpful to work through the pain, but this is not always the case. Note that your aim should always be to feel better than when you started exercising, or at least to end feeling good overall.

Referring again to our right shoulder injury model, one of the things that can retain strength in the injured arm is performing strength work with your uninjured arm. Your nervous system is very adaptive; one of its interesting adaptations is the phenomena of cross education. When a unilaterally trained skill or strength movement is performed with the opposite limb, strength benefits are transferred, even if that particular limb has not practiced the skill or performed any strength work. Performing unilateral work with your uninjured left arm will benefit your injured right arm.
As an experiment, if you normally throw a hall or dribble a basketball with your left arm, practice throwing or dribbling with your right arm. After a significant unilateral practice, test your left arm. You should be able to dribble better or throw the hall farther without having practiced on that arm at all.
Studies show that the transfer of strength to the opposite limb from cross education is around 5-10%. While this is not much, it is still very beneficial, especially if your injury sets you back more than two weeks. At this point, your body is at risk for muscle atrophy and rapid decrease in neurological strength. Retainingas much strength and stability as possible is criticalfor speedy recovery.
You do need to take care toensurethatno imbalances develop between uninjured and injured limbs. This can be accomplished by maintaining a low volume and fairly high intensity level, similar to typical strength work. Aim for a few sets of three to six repetitions with the opposite arm if you are going to perform unilateral work. Unaffected limbs and Other Areas
After exhausting all options with your injured limb and the opposing limb, you still need to continue working the rest of your body. Some types of full-body exercises like squats and deadlifts may interfere with proper healing. Any exercise that irritates your injury should be avoided until you recover.
This is a great opportunity to work on specific weaknesses that do not interact with your injured right shoulder (to use our model). For example, if you know you have cight hamstrings or a tight back, you can improve these mobility limitations while you are recovering from your injury. This is especially important if flexibility and mobility are lagging behind in certain skills like press handstand, V-sit or manna-type work. For your legs, it may be better to focus on light-intensity exercises to help improve your heart rate and blood flow, as this will accelerate the healing process. Pursue balance and agilicy work. If your injury is in your lower body you might be able to focus on handstands or rings strength. Work on as many weaknesses as you can without impeding the injury recovery process. Do not allow an injury to steal your motivation; let it be a learning experience and opportunity to work on your weaknesses so you can come back stronger than ever.
When it comes to findinga good medical professional, you should look for a well-qualifled orthopedic doctor, physical therapist, or chiropractor that really listens to your situation and connects with your personality.
While there are some massage therapists and personal trainers who know a lot about injuries, this is the exception. Find a professional who works specifically with athletes. medical professionals will specialize in different things, especially orthopedic doctors. Some work specifically with the lower body, some with the upper body. There are shoulder specialists, knee specialists, and so
forth. It is less important to find the specialist for your exact injury than to find one that works with athletes and has a good reputation. As the saying goes, the cream of the crop rises to the top. These tend to work with college or high school athletic teams and have extensive knowledge of orthopedic injuries and treatment options based on the severity of the injury. Here is a threefold plan for choosing a qualifled medical professional:
Good medical professionals should be able to explain not only why they are performing particular treatments and but also the methodology behind them. If you have any question about a specific treatment, ask them directly. Learn to think critically about your body.
Welcome to the world of exercise, where everyone has an opinion on everything. To learn how to discern between "good" and "bad" exercises, follow these steps:
For example, in terms of shoulder injury risk, one-arm chin-ups are potentially a "worse" exercise compared to weighted pull-ups. This is because in the former, you must control the torqueing movement that is not present with two-handed pull-ups. If the torque is not properly controlled it can lead to rotator cuff dysfunction, tendonitis, or a similar injury.
For something to be "bad" it has to be compared to something else. If someone says a particular exercise is bad, they should be able to suggest a better exercise you can perform instead. Likewise, "good" must be relative to a specific goal. If training for one-arm chin-ups by performing certain exercises is contraindicated, there are other exercises you can use. There is more than one way to reach most goals and exercises fall on a spectrum of good, bad, and everything in between.
Using the above example, the mechanism of potential injury is the relative control of the torque at the shoulder. However, you must control torque with any exercise. It is more accurate to say that a one-arm chin-up performed without adequate preparation for effective control is a bad move, rather than labeling the movement itself as bad. For things like squats with a rounded back, the rounded back may increase your risk of injury because the fluid in the clise will start to put posterior pressure on the lamina! fibers, which may cause bulging or herniation of the clises. However, rounded back squats or deadlifts can be successfully built up to where there is minimal risk of injury.

Anecdotal evidence and experience counts for some. A coach's story about a patient who randomly hurt their arm doing X is one data point. However, if there are stories of one hundred people hurting their arms doingX the advice tends to be credible. The same is true of research. If research backs up the experience of one hundred people hurting their arms in the same manner, it is safe to label that experience as "bad" for that particular method.
Let's say you have only met a few people who have injured themselves performing kipping pull-ups (not much experience) and there is not a lot of research on the amount of force that kipping pull-ups place on the shoulders (not much data). However, you know there is a mechanism of injury wherein a heavily fatigued body dropping into the bottom of a pull-up position can cause rotator cuffor even labrum injury. This rate of injury appears to be higher in those performing kipping pull-ups than those performing standard pull-ups.
You can therefore logically condude that kipping pull-ups carry a higher rate of injury than standard pull-ups, even though you do not have much experience or research to back it up. In light of this, a good coach would advise beginners or those who are more prone to injury to avoid kipping pull-ups when they are just starting out. This doesn't mean kipping pull-ups are inherendy a bad exercise-though they would certainly be bad be under certain conditions, such as with beginners (because they have not yet learned proper technique), with those who have previously injured their shoulders, and with athletes who are fatigued.
Exercise is always a cost-benefit assessment. One might perform the most dangerous exercises in the world and never get injured. A cost-benefit assessment looks at exercises as tools. A chain saw is a great tool for cutting, but carries some inherent risk of injury, whereas a power saw or hand saw is less dangerous but also less effective. All exercises bring with them a tension of risk vs. reward, some more than others. If an exercise is considered "dangerous" you may want to avoid it until you are more experienced. Research your exercises so you can be informed of any inherent dangers, and plan accordingly. This is where critical thinking comes in.
Always fact check. There could be a mechanism of injury that sounds logical but is false. Science has known for some time that a gluten allergy is a celiac disease, but has recendy discovered that gluten insensitivity appears not to exist. In light of this, one could ask why eating gluten is ever detrimental for people who don't have celiac disease?
(The answer may partially lie in other research such as FODMAPs-fermentable oligo-, di-, monosaccharides and polyols. Those who remove FODMAPs from their diet due to irritable bowel syndrome and other gastrointestinal distress issues may show marked increases in how well they feel and perform. Even though "gluten insensitivity" may be a misnomer, this does not mean certain foods do not cause the symptoms. Wheat and other grain products in particular tend to have a lot of fructans, galactans, and polyols, all of which may irritate the bowels.)
To review:
Propensity for overuse, pain location, tissue qualicy, poscure and positioning, and biomechanics all play critical roles in the development of an injury, either acute or chronic. Even if you have a good idea of what your injury is, have a qualified medical professional check it out.
A general evaluation of the circumstances surrounding any injury brings one to the conclusion that it is always best to see a medical professional for a diagnosis. Once you have a diagnosis, you can direccly address the cause of the injury, allowing for fascer recovery. If a solucion is not readily available, it may be necessary to ucilize the "wait and see" approach, chough this is not preferred.
A chronological treatment of injury will allow for work on concepts such as protection from atrophy, range of motion, strength, etc. during the inflammatory, proliferation, and remodeling phases. There are particular loading, repetitions, sets, and volume for rehabilitating specific injuries. Each injury needs to be addressed wichin the context of its severity and interference with normal bodily function. Most types of injuries can be addressed with light, controlled, eccentric exercises. High repetitions tend to work best.
It is possible to effectively and safely program around injuries using the methods of intra-limb exercises, opposite limb exercises, and exercising in unaffected areas. lntra-limb exercises on unaffected areas help maintain the strength and mobility of uninjured tissues. Opposite-limb exercises assist by the theory of cross education. Exercising in unaffected areas assists with blood flow and overall well-being.
Always perform rehabilitation workfaryour injuries instead of avoiding them by programming other types of exercises to compensate.
In situations of non-critical injuries, the traditional RICE approach is less effective than the newer MEAT approach. Methods to find a good medical professional and how to approach good/bad exercises by chinking critically were also covered.
Previous Chapter ... ... Next Chapter